
Page 30 - Laparoscopic Surgery Online Journal
P. 30
Aswini Kumar Misro et al
take the abdominal wall further away from the abdominal
viscera. The stab wound should not be widened further as it
is easy to maintain good air seal around a small wound.
If the hemostat is going inside the peritoneal cavity without
any undue resistance peritoneal access is almost certain.
However, if the incision is too much away from the umbilical
tube and sheath junction, a separate posterior sheath may
be encountered. In this situation, one option is to dissect
and incise the posterior sheath as well. Other option is to
start fresh at the junction closing the former wound. The
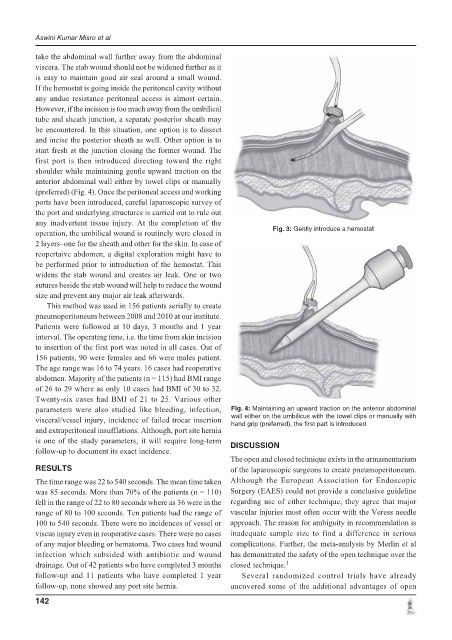
first port is then introduced directing toward the right
shoulder while maintaining gentle upward traction on the
anterior abdominal wall either by towel clips or manually
(preferred) (Fig. 4). Once the peritoneal access and working
ports have been introduced, careful laparoscopic survey of
the port and underlying structures is carried out to rule out
any inadvertent tissue injury. At the completion of the
Fig. 3: Gently introduce a hemostat
operation, the umbilical wound is routinely were closed in
2 layers–one for the sheath and other for the skin. In case of
reopertaive abdomen, a digital exploration might have to
be performed prior to introduction of the hemostat. This
widens the stab wound and creates air leak. One or two
sutures beside the stab wound will help to reduce the wound
size and prevent any major air leak afterwards.
This method was used in 156 patients serially to create
pneumoperitoneum between 2008 and 2010 at our institute.
Patients were followed at 10 days, 3 months and 1 year
interval. The operating time, i.e. the time from skin incision
to insertion of the first port was noted in all cases. Out of
156 patients, 90 were females and 66 were males patient.
The age range was 16 to 74 years. 16 cases had reoperative
abdomen. Majority of the patients (n = 115) had BMI range
of 26 to 29 where as only 10 cases had BMI of 30 to 32.
Twenty-six cases had BMI of 21 to 25. Various other
parameters were also studied like bleeding, infection, Fig. 4: Maintaining an upward traction on the anterior abdominal
wall either on the umbilicus with the towel clips or manually with
visceral/vessel injury, incidence of failed trocar insertion
hand grip (preferred), the first part is introduced
and extraperitoneal insufflations. Although, port site hernia
is one of the study parameters, it will require long-term
DISCUSSION
follow-up to document its exact incidence.
The open and closed technique exists in the armamentarium
RESULTS of the laparoscopic surgeons to create pneumoperitoneum.
The time range was 22 to 540 seconds. The mean time taken Although the European Association for Endoscopic
was 85 seconds. More than 70% of the patients (n = 110) Surgery (EAES) could not provide a conclusive guideline
fell in the range of 22 to 80 seconds where as 36 were in the regarding use of either technique, they agree that major
range of 80 to 100 seconds. Ten patients had the range of vascular injuries most often occur with the Veress needle
100 to 540 seconds. There were no incidences of vessel or approach. The reason for ambiguity in recommendation is
viscus injury even in reoperative cases. There were no cases inadequate sample size to find a difference in serious
of any major bleeding or hematoma. Two cases had wound complications. Further, the meta-analysis by Merlin et al
infection which subsided with antibiotic and wound has demonstrated the safety of the open technique over the
drainage. Out of 42 patients who have completed 3 months closed technique. 1
follow-up and 11 patients who have completed 1 year Several randomized control trials have already
follow-up, none showed any port site hernia. uncovered some of the additional advantages of open
142