
Page 29 - Laparoscopic Surgery Online Journal
P. 29
WJOLS
10.5005/jp-journals-10033-1201
Our Experience of Open Technique of Creating Pneumoperitoneum through Umbilical Cicatrix from a Remote Health Facility
ORIGINAL ARTICLE
Our Experience of Open Technique of Creating
Pneumoperitoneum through Umbilical Cicatrix
from a Remote Health Facility at Nepal
Aswini Kumar Misro, Prakash Sapkota, Radhika Misro
ABSTRACT subumbilical or supraumbilical position depending on the
Background: Two methods have been used for peritoneal operation contemplated. After careful hemostasis, the
access to create pnemoperitoneum–the open and the closed incision is deepened till the portion of the umbilical tube
technique. We are describing here an open technique of joining the linea alba is exposed and suitable retraction is
creating pneumoperitoneum through the umbilical cicatrix. We
have been using this technique routinely in view of its safety, applied to maintain this position and field of vision. With a
rapidity and technical ease. no. 15 blade a small incision of around 5 mm is taken on
the junction (Fig. 2). Care should be taken at this stage to
Materials and methods: This method was used in 156 patients
serially to create pneumoperitoneum. Patients were followed complete this step under vision without introducing the blade
at 10 days, 3 months and 1 year interval. too much inside. A blunt tipped hemostat is gently
Results: The time range was 22 to 540 seconds. The mean introduced through the incision (Fig. 3). A gushing noise
time taken was 85 seconds. More than 70% of the patients can be heard at this juncture due to air entry inside the
(n = 110) fell in the range of 22 to 80 seconds where as 36 peritoneal cavity. This will widen the peritoneal space and
were in the range of 80 to 100 seconds. Ten patients had the
range of 100 to 540 seconds. There were no incidences of
vessel or viscus injury even in reoperative cases. There were
no cases of any major bleeding or hematoma. Two cases had
wound infection which subsided with antibiotic and wound
drainage. Out of 42 patients who have completed 3 months
follow-up and 11 patients who have completed 1 year follow-
up, none showed any port site hernia.
Conclusion: The open technique of creating pneumoperitoneum
through the umbilical cicatrix is a safe and rapid technique.
Keywords: Open, Pneumoperitoneum, Laparoscopy, Umbilicus.
How to cite this article: Misro AK, Sapkota P, Misro R. Our
Experience of Open Technique of Creating Pneumoperitoneum
through Umbilical Cicatrix from a Remote Health Facility at
Nepal. World J Lap Surg 2013;6(3):141-143.
Source of support: Nil
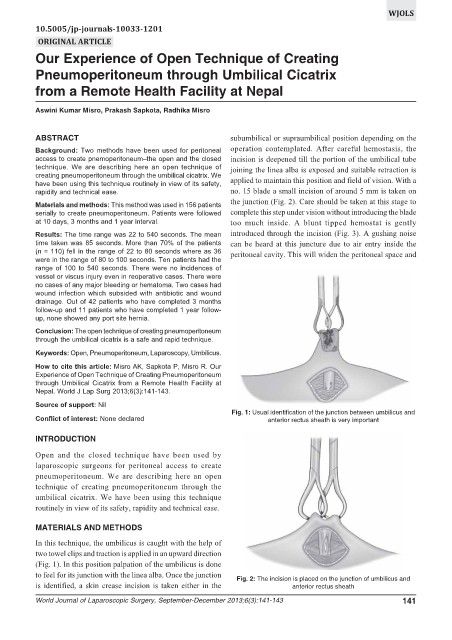
Fig. 1: Usual identification of the junction between umbilicus and
Conflict of interest: None declared anterior rectus sheath is very important
INTRODUCTION
Open and the closed technique have been used by
laparoscopic surgeons for peritoneal access to create
pneumoperitoneum. We are describing here an open
technique of creating pneumoperitoneum through the
umbilical cicatrix. We have been using this technique
routinely in view of its safety, rapidity and technical ease.
MATERIALS AND METHODS
In this technique, the umbilicus is caught with the help of
two towel clips and traction is applied in an upward direction
(Fig. 1). In this position palpation of the umbilicus is done
to feel for its junction with the linea alba. Once the junction
Fig. 2: The incision is placed on the junction of umbilicus and
is identified, a skin crease incision is taken either in the anterior rectus sheath
World Journal of Laparoscopic Surgery, September-December 2013;6(3):141-143 141