
Page 50 - World Journal of Laparoscopic Surgery
P. 50
Laparoscopic Diaphragmatic Repair
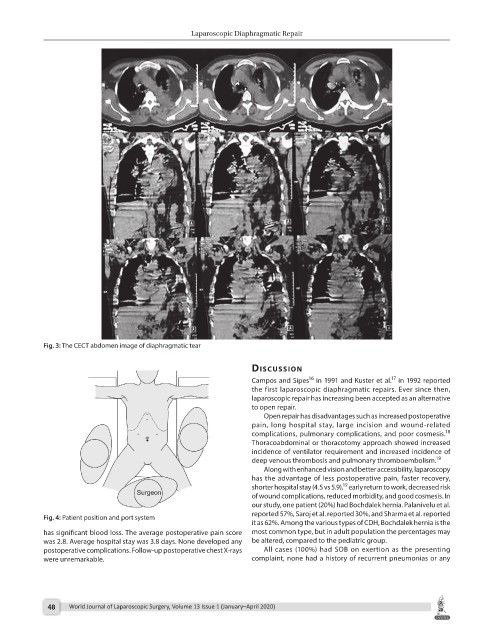
Fig. 3: The CECT abdomen image of diaphragmatic tear
dIscussIon
16
17
Campos and Sipes in 1991 and Kuster et al. in 1992 reported
the first laparoscopic diaphragmatic repairs. Ever since then,
laparoscopic repair has increasing been accepted as an alternative
to open repair.
Open repair has disadvantages such as increased postoperative
pain, long hospital stay, large incision and wound-related
18
complications, pulmonary complications, and poor cosmesis.
Thoracoabdominal or thoracotomy approach showed increased
incidence of ventilator requirement and increased incidence of
deep venous thrombosis and pulmonary thromboembolism. 19
Along with enhanced vision and better accessibility, laparoscopy
has the advantage of less postoperative pain, faster recovery,
19
shorter hospital stay (4.5 vs 5.9), early return to work, decreased risk
of wound complications, reduced morbidity, and good cosmesis. In
our study, one patient (20%) had Bochdalek hernia. Palanivelu et al.
reported 57%, Saroj et al. reported 30%, and Sharma et al. reported
Fig. 4: Patient position and port system
it as 62%. Among the various types of CDH, Bochdalek hernia is the
has significant blood loss. The average postoperative pain score most common type, but in adult population the percentages may
was 2.8. Average hospital stay was 3.8 days. None developed any be altered, compared to the pediatric group.
postoperative complications. Follow-up postoperative chest X-rays All cases (100%) had SOB on exertion as the presenting
were unremarkable. complaint, none had a history of recurrent pneumonias or any
48 World Journal of Laparoscopic Surgery, Volume 13 Issue 1 (January–April 2020)