
Page 12 - World Journal of Laparoscopic Surgery
P. 12
Nuhu Musa Mshelia et al
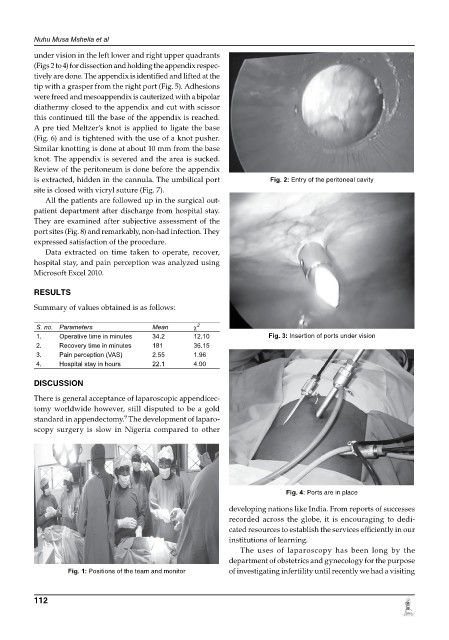
under vision in the left lower and right upper quadrants
(Figs 2 to 4) for dissection and holding the appendix respec-
tively are done. The appendix is identified and lifted at the
tip with a grasper from the right port (Fig. 5). Adhesions
were freed and mesoappendix is cauterized with a bipolar
diathermy closed to the appendix and cut with scissor
this continued till the base of the appendix is reached.
A pre tied Meltzer’s knot is applied to ligate the base
(Fig. 6) and is tightened with the use of a knot pusher.
Similar knotting is done at about 10 mm from the base
knot. The appendix is severed and the area is sucked.
Review of the peritoneum is done before the appendix
is extracted, hidden in the cannula. The umbilical port Fig. 2: Entry of the peritoneal cavity
site is closed with vicryl suture (Fig. 7).
All the patients are followed up in the surgical out-
patient department after discharge from hospital stay.
They are examined after subjective assessment of the
port sites (Fig. 8) and remarkably, non-had infection. They
expressed satisfaction of the procedure.
Data extracted on time taken to operate, recover,
hospital stay, and pain perception was analyzed using
Microsoft Excel 2010.
RESuLTS
Summary of values obtained is as follows:
2
S. no. Parameters Mean c
1. Operative time in minutes 34.2 12.10 Fig. 3: Insertion of ports under vision
2. Recovery time in minutes 181 36.15
3. Pain perception (VAS) 2.55 1.96
4. Hospital stay in hours 22.1 4.00
dISCuSSION
There is general acceptance of laparoscopic appendic ec -
tomy worldwide however, still disputed to be a gold
9
standard in appendectomy. The development of laparo-
scopy surgery is slow in Nigeria compared to other
Fig. 4: Ports are in place
developing nations like India. From reports of successes
recorded across the globe, it is encouraging to dedi-
cated resources to establish the services efficiently in our
institutions of learning.
The uses of laparoscopy has been long by the
department of obstetrics and gynecology for the purpose
Fig. 1: Positions of the team and monitor of investigating infertility until recently we had a visiting
112