
Page 26 - WJOLS - Laparoscopic Journal
P. 26
Inamull Hasan SA Shaikh
• An area of fibrosis develops around the anastomosis But, the learning curve for laparoscopic colorectal
and the sacrum which leads to a rectal fixation to the surgery has been found to be around 150 to 200 cases
sacrum for achieving a constant level of proficiency. 17,18 This also
• The colon lies in a straighter course which avoids seems to apply to laparoscopic rectopexy.
torsion and sigmoidocele. 14
Especially in patients with an elongated sigmoid and COMPARISON OF LAPAROSCOPIC
slow-transit constipation it is postulated that constipation AND OPEN PROCEDURES
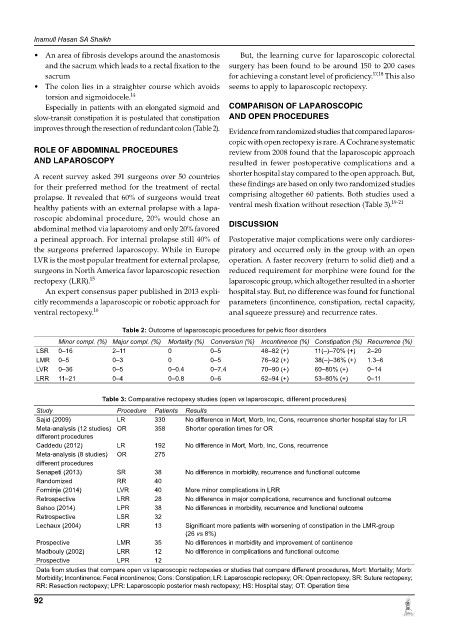
improves through the resection of redundant colon (Table 2). Evidence from randomized studies that compared laparos-
copic with open rectopexy is rare. A Cochrane systematic
ROLE OF ABDOMINAL PROCEDURES review from 2008 found that the laparoscopic approach
AND LAPAROSCOPY resulted in fewer postoperative complications and a
A recent survey asked 391 surgeons over 50 countries shorter hospital stay compared to the open approach. But,
for their preferred method for the treatment of rectal these findings are based on only two randomized studies
prolapse. It revealed that 60% of surgeons would treat comprising altogether 60 patients. Both studies used a
healthy patients with an external prolapse with a lapa- ventral mesh fixation without resection (Table 3). 19-21
roscopic abdominal procedure, 20% would chose an
abdominal method via laparotomy and only 20% favored DISCUSSION
a perineal approach. For internal prolapse still 40% of Postoperative major complications were only cardiores-
the surgeons preferred laparoscopy. While in Europe piratory and occurred only in the group with an open
LVR is the most popular treatment for external prolapse, operation. A faster recovery (return to solid diet) and a
surgeons in North America favor laparoscopic resection reduced requirement for morphine were found for the
rectopexy (LRR). 15 laparoscopic group, which altogether resulted in a shorter
An expert consensus paper published in 2013 expli- hospital stay. But, no difference was found for functional
citly recommends a laparoscopic or robotic approach for parameters (incontinence, constipation, rectal capacity,
ventral rectopexy. 16 anal squeeze pressure) and recurrence rates.
Table 2: Outcome of laparoscopic procedures for pelvic floor disorders
Minor compl. (%) Major compl. (%) Mortality (%) Conversion (%) Incontinence (%) Constipation (%) Recurrence (%)
LSR 0–16 2–11 0 0–5 48–82 (+) 11(–)–70% (+) 2–20
LMR 0–5 0–3 0 0–5 76–92 (+) 38(–)–36% (+) 1.3–6
LVR 0–36 0–5 0–0.4 0–7.4 70–90 (+) 60–80% (+) 0–14
LRR 11–21 0–4 0–0.8 0–6 62–94 (+) 53–80% (+) 0–11
Table 3: Comparative rectopexy studies (open vs laparoscopic, different procedures)
Study Procedure Patients Results
Sajid (2009) LR 330 No difference in Mort, Morb, Inc, Cons, recurrence shorter hospital stay for LR
Meta-analysis (12 studies) OR 358 Shorter operation times for OR
different procedures
Caddedu (2012) LR 192 No difference in Mort, Morb, Inc, Cons, recurrence
Meta-analysis (8 studies) OR 275
different procedures
Senapeti (2013) SR 38 No difference in morbidity, recurrence and functional outcome
Randomized RR 40
Forminje (2014) LVR 40 More minor complications in LRR
Retrospective LRR 28 No difference in major complications, recurrence and functional outcome
Sahoo (2014) LPR 38 No differences in morbidity, recurrence and functional outcome
Retrospective LSR 32
Lechaux (2004) LRR 13 Significant more patients with worsening of constipation in the LMR-group
(26 vs 8%)
Prospective LMR 35 No differences in morbidity and improvement of continence
Madbouly (2002) LRR 12 No difference in complications and functional outcome
Prospective LPR 12
Data from studies that compare open vs laparoscopic rectopexies or studies that compare different procedures, Mort: Mortality; Morb:
Morbidity; Incontinence: Fecal incontinence; Cons: Constipation; LR: Laparoscopic rectopexy; OR: Open rectopexy; SR: Suture rectopexy;
RR: Resection rectopexy; LPR: Laparoscopic posterior mesh rectopexy; HS: Hospital stay; OT: Operation time
92