
Page 25 - WJOLS - Laparoscopic Journal
P. 25
WJOLS
Surgical Approaches for Rectal Prolapse and their Comparative Study
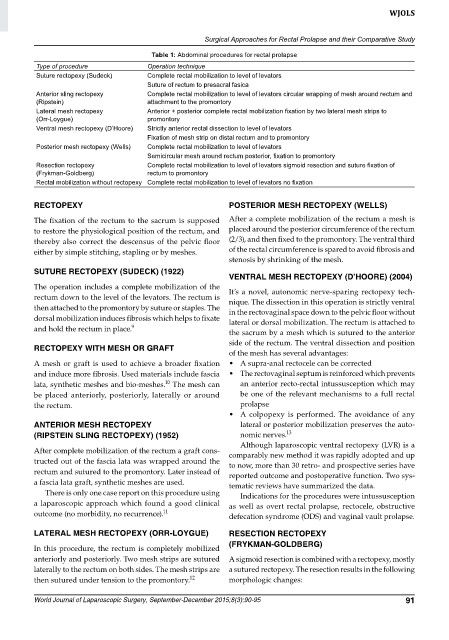
Table 1: Abdominal procedures for rectal prolapse
Type of procedure Operation technique
Suture rectopexy (Sudeck) Complete rectal mobilization to level of levators
Suture of rectum to presacral fasica
Anterior sling rectopexy Complete rectal mobilization to level of levators circular wrapping of mesh around rectum and
(Ripstein) attachment to the promontory
Lateral mesh rectopexy Anterior + posterior complete rectal mobilization fixation by two lateral mesh strips to
(Orr-Loygue) promontory
Ventral mesh rectopexy (D’Hoore) Strictly anterior rectal dissection to level of levators
Fixation of mesh strip on distal rectum and to promontory
Posterior mesh rectopexy (Wells) Complete rectal mobilization to level of levators
Semicircular mesh around rectum posterior, fixation to promontory
Resection rectopexy Complete rectal mobilization to level of levators sigmoid resection and suture fixation of
(Frykman-Goldberg) rectum to promontory
Rectal mobilization without rectopexy Complete rectal mobilization to level of levators no fixation
RECTOPEXY POSTERIOR MESH RECTOPEXY (WELLS)
The fixation of the rectum to the sacrum is supposed After a complete mobilization of the rectum a mesh is
to restore the physiological position of the rectum, and placed around the posterior circumference of the rectum
thereby also correct the descensus of the pelvic floor (2/3), and then fixed to the promontory. The ventral third
either by simple stitching, stapling or by meshes. of the rectal circumference is spared to avoid fibrosis and
stenosis by shrinking of the mesh.
SUTURE RECTOPEXY (SUDECK) (1922)
VENTRAL MESH RECTOPEXY (D’HOORE) (2004)
The operation includes a complete mobilization of the It’s a novel, autonomic nerve-sparing rectopexy tech-
rectum down to the level of the levators. The rectum is nique. The dissection in this operation is strictly ventral
then attached to the promontory by suture or staples. The in the rectovaginal space down to the pelvic floor without
dorsal mobilization induces fibrosis which helps to fixate lateral or dorsal mobilization. The rectum is attached to
and hold the rectum in place. 9
the sacrum by a mesh which is sutured to the anterior
side of the rectum. The ventral dissection and position
RECTOPEXY WITH MESH OR GRAFT
of the mesh has several advantages:
A mesh or graft is used to achieve a broader fixation • A supra-anal rectocele can be corrected
and induce more fibrosis. Used materials include fascia • The rectovaginal septum is reinforced which prevents
10
lata, synthetic meshes and bio-meshes. The mesh can an anterior recto-rectal intussusception which may
be placed anteriorly, posteriorly, laterally or around be one of the relevant mechanisms to a full rectal
the rectum. prolapse
• A colpopexy is performed. The avoidance of any
ANTERIOR MESH RECTOPEXY lateral or posterior mobilization preserves the auto-
(RIPSTEIN SLING RECTOPEXY) (1952) nomic nerves. 13
Although laparoscopic ventral rectopexy (LVR) is a
After complete mobilization of the rectum a graft cons- comparably new method it was rapidly adopted and up
tructed out of the fascia lata was wrapped around the to now, more than 30 retro- and prospective series have
rectum and sutured to the promontory. Later instead of reported outcome and postoperative function. Two sys-
a fascia lata graft, synthetic meshes are used. tematic reviews have summarized the data.
There is only one case report on this procedure using Indications for the procedures were intussusception
a laparoscopic approach which found a good clinical as well as overt rectal prolapse, rectocele, obstructive
outcome (no morbidity, no recurrence). 11 defecation syndrome (ODS) and vaginal vault prolapse.
LATERAL MESH RECTOPEXY (ORR-LOYGUE) RESECTION RECTOPEXY
(FRYKMAN-GOLDBERG)
In this procedure, the rectum is completely mobilized
anteriorly and posteriorly. Two mesh strips are sutured A sigmoid resection is combined with a rectopexy, mostly
laterally to the rectum on both sides. The mesh strips are a sutured rectopexy. The resection results in the following
then sutured under tension to the promontory. 12 morphologic changes:
World Journal of Laparoscopic Surgery, September-December 2015;8(3):90-95 91