
Page 32 - wjols
P. 32
CASE REPORT
Laparoscopic Retrieval of a Migrated Intrauterine
Contraceptive Device
1
Eftekhar Hassan Al-Ojaimi , Shafeeqa Ali Ebrahim 2
AbstrAct
Introduction: Intrauterine contraceptive device (IUCD) migration consequent to perforation of the uterus is not very common, but is one of
the more serious complications.
Case descriptions: We described two cases of migrated IUCD, at two distinct sites in the pelvic cavity, one was located in the pouch of Douglas
embedded behind the left ovary and tube which was adherent to the posterior uterine wall and another was in the left mesovarium between
the ovary and the tube. Both IUCDs were successfully removed laparoscopically without any complication.
Conclusion: Migrated IUCDs should always be removed once the diagnosis is made to prevent serious complications. Laparoscopic approach
is a successful and preferred choice of treatment in selected cases.
Keywords: Intrauterine device, Laparoscopy, Migration, Uterine perforation.
World Journal of Laparoscopic Surgery (2020): 10.5005/jp-journals-10033-1409
IntroductIon 1 Department of Obstetrics and Gynecology, Al Zahra Hospital Dubai,
Intrauterine contraceptive device (IUCD) is one of the most widely Dubai, United Arab Emirates
used forms of contraception, predominantly in the developing 2 Department of Obstetrics and Gynecology, Salmaniya Medical
countries. This method has the benefits in terms of affordability, as Complex, Ministry of Health, Kingdom of Bahrain
also being very effective, long-lasting, and reversible but it is not Corresponding Author: Eftekhar Hassan Al-Ojaimi, Department of
risk free. Insertion of an IUCD is associated with some complications Obstetrics and Gynecology, Al Zahra Hospital Dubai, Dubai, United
like cramping abdominal pain, irregular and sometimes heavy Arab Emirates, Phone: +971566608555, e-mail: eojaimi@gmail.com
vaginal bleeding, expulsion, and even serious complications, such How to cite this article: Hassan Al-Ojaimi E, Ebrahim SA. Laparoscopic
as infection and pelvic inflammatory disease, retraction back to the Retrieval of a Migrated Intrauterine Contraceptive Device. World J Lap
1,2
cervix or uterine cavity, and subsequent uterine perforation. The Surg 2020;13(2):84–86.
incidence of uterine wall perforations is estimated to be around Source of support: Nil
2
0.2–9.6 per thousand insertions. A migrated IUCD can be found Conflict of interest: None
in different positions in the pelvic or abdominal cavity, which
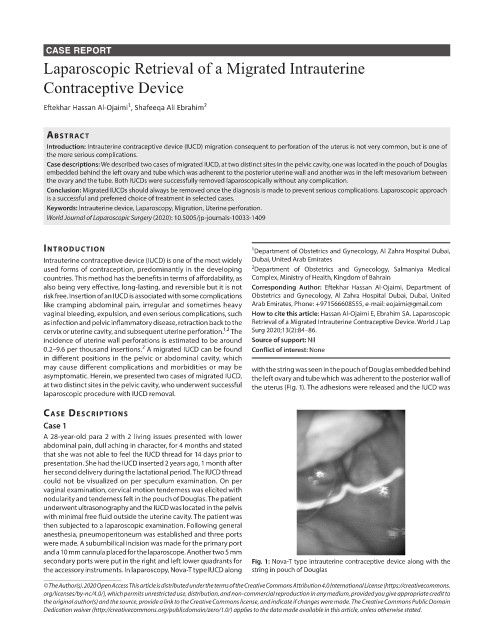
may cause different complications and morbidities or may be with the string was seen in the pouch of Douglas embedded behind
asymptomatic. Herein, we presented two cases of migrated IUCD, the left ovary and tube which was adherent to the posterior wall of
at two distinct sites in the pelvic cavity, who underwent successful the uterus (Fig. 1). The adhesions were released and the IUCD was
laparoscopic procedure with IUCD removal.
cAse descrIptIons
Case 1
A 28-year-old para 2 with 2 living issues presented with lower
abdominal pain, dull aching in character, for 4 months and stated
that she was not able to feel the IUCD thread for 14 days prior to
presentation. She had the IUCD inserted 2 years ago, 1 month after
her second delivery during the lactational period. The IUCD thread
could not be visualized on per speculum examination. On per
vaginal examination, cervical motion tenderness was elicited with
nodularity and tenderness felt in the pouch of Douglas. The patient
underwent ultrasonography and the IUCD was located in the pelvis
with minimal free fluid outside the uterine cavity. The patient was
then subjected to a laparoscopic examination. Following general
anesthesia, pneumoperitoneum was established and three ports
were made. A subumbilical incision was made for the primary port
and a 10 mm cannula placed for the laparoscope. Another two 5 mm
secondary ports were put in the right and left lower quadrants for Fig. 1: Nova-T type intrauterine contraceptive device along with the
the accessory instruments. In laparoscopy, Nova-T type IUCD along string in pouch of Douglas
© The Author(s). 2020 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.
org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to
the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain
Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.