
Page 29 - wjols
P. 29
Laparoscopic Heminephroureterectomy in Infants Weighing Less Than 10 Kilograms
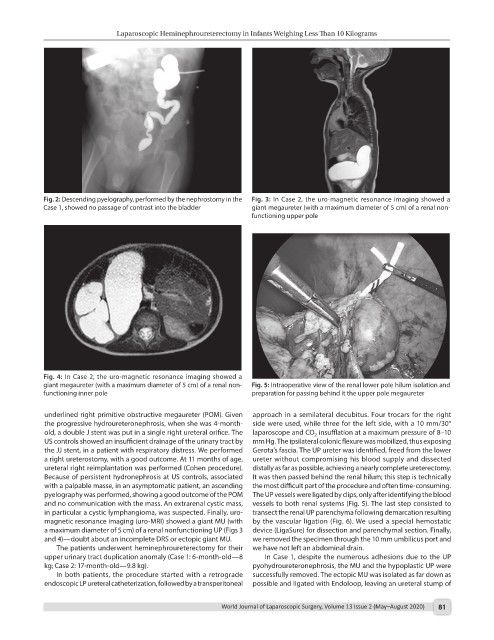
Fig. 2: Descending pyelography, performed by the nephrostomy in the Fig. 3: In Case 2, the uro-magnetic resonance imaging showed a
Case 1, showed no passage of contrast into the bladder giant megaureter (with a maximum diameter of 5 cm) of a renal non-
functioning upper pole
Fig. 4: In Case 2, the uro-magnetic resonance imaging showed a
giant megaureter (with a maximum diameter of 5 cm) of a renal non- Fig. 5: Intraoperative view of the renal lower pole hilum isolation and
functioning inner pole preparation for passing behind it the upper pole megaureter
underlined right primitive obstructive megaureter (POM). Given approach in a semilateral decubitus. Four trocars for the right
the progressive hydroureteronephrosis, when she was 4-month- side were used, while three for the left side, with a 10 mm/30°
old, a double J stent was put in a single right ureteral orifice. The laparoscope and CO insufflation at a maximum pressure of 8–10
2
US controls showed an insufficient drainage of the urinary tract by mm Hg. The ipsilateral colonic flexure was mobilized, thus exposing
the JJ stent, in a patient with respiratory distress. We performed Gerota’s fascia. The UP ureter was identified, freed from the lower
a right ureterostomy, with a good outcome. At 11 months of age, ureter without compromising his blood supply and dissected
ureteral right reimplantation was performed (Cohen procedure). distally as far as possible, achieving a nearly complete ureterectomy.
Because of persistent hydronephrosis at US controls, associated It was then passed behind the renal hilum; this step is technically
with a palpable masse, in an asymptomatic patient, an ascending the most difficult part of the procedure and often time-consuming.
pyelography was performed, showing a good outcome of the POM The UP vessels were ligated by clips, only after identifying the blood
and no communication with the mass. An extrarenal cystic mass, vessels to both renal systems (Fig. 5). The last step consisted to
in particular a cystic lymphangioma, was suspected. Finally, uro- transect the renal UP parenchyma following demarcation resulting
magnetic resonance imaging (uro-MRI) showed a giant MU (with by the vascular ligation (Fig. 6). We used a special hemostatic
a maximum diameter of 5 cm) of a renal nonfunctioning UP (Figs 3 device (LigaSure) for dissection and parenchymal section. Finally,
and 4)—doubt about an incomplete DRS or ectopic giant MU. we removed the specimen through the 10 mm umbilicus port and
The patients underwent heminephroureterectomy for their we have not left an abdominal drain.
upper urinary tract duplication anomaly (Case 1: 6-month-old—8 In Case 1, despite the numerous adhesions due to the UP
kg; Case 2: 17-month-old—9.8 kg). pyohydroureteronephrosis, the MU and the hypoplastic UP were
In both patients, the procedure started with a retrograde successfully removed. The ectopic MU was isolated as far down as
endoscopic LP ureteral catheterization, followed by a transperitoneal possible and ligated with Endoloop, leaving an ureteral stump of
World Journal of Laparoscopic Surgery, Volume 13 Issue 2 (May–August 2020) 81