
Page 36 - wjols
P. 36
Laparoscopic Retrieval of a Displaced IUD
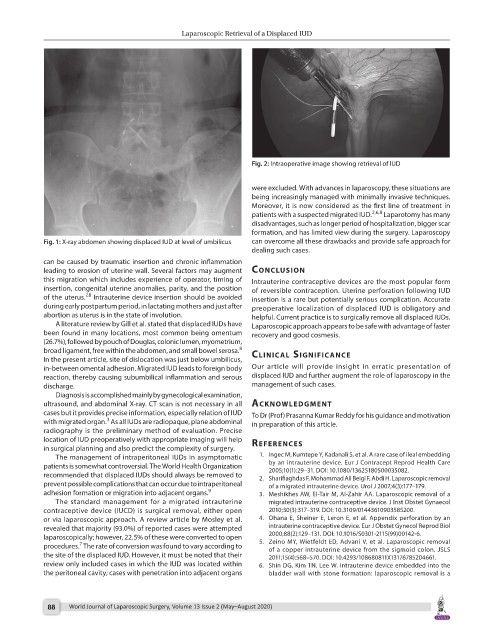
Fig. 2: Intraoperative image showing retrieval of IUD
were excluded. With advances in laparoscopy, these situations are
being increasingly managed with minimally invasive techniques.
Moreover, it is now considered as the first line of treatment in
patients with a suspected migrated IUD. 2,6,8 Laparotomy has many
disadvantages, such as longer period of hospitalization, bigger scar
formation, and has limited view during the surgery. Laparoscopy
Fig. 1: X-ray abdomen showing displaced IUD at level of umbilicus can overcome all these drawbacks and provide safe approach for
dealing such cases.
can be caused by traumatic insertion and chronic inflammation
leading to erosion of uterine wall. Several factors may augment conclusion
this migration which includes experience of operator, timing of Intrauterine contraceptive devices are the most popular form
insertion, congenital uterine anomalies, parity, and the position of reversible contraception. Uterine perforation following IUD
7,8
of the uterus. Intrauterine device insertion should be avoided insertion is a rare but potentially serious complication. Accurate
during early postpartum period, in lactating mothers and just after preoperative localization of displaced IUD is obligatory and
abortion as uterus is in the state of involution. helpful. Current practice is to surgically remove all displaced IUDs.
A literature review by Gill et al. stated that displaced IUDs have Laparoscopic approach appears to be safe with advantage of faster
been found in many locations, most common being omentum recovery and good cosmesis.
(26.7%), followed by pouch of Douglas, colonic lumen, myometrium,
8
broad ligament, free within the abdomen, and small bowel serosa. clinicAl significAnce
In the present article, site of dislocation was just below umbilicus,
in-between omental adhesion. Migrated IUD leads to foreign body Our article will provide insight in erratic presentation of
reaction, thereby causing subumbilical inflammation and serous displaced IUD and further augment the role of laparoscopy in the
discharge. management of such cases.
Diagnosis is accomplished mainly by gynecological examination,
ultrasound, and abdominal X-ray. CT scan is not necessary in all Acknowledgment
cases but it provides precise information, especially relation of IUD To Dr (Prof) Prasanna Kumar Reddy for his guidance and motivation
3
with migrated organ. As all IUDs are radiopaque, plane abdominal in preparation of this article.
radiography is the preliminary method of evaluation. Precise
location of IUD preoperatively with appropriate imaging will help references
in surgical planning and also predict the complexity of surgery.
The management of intraperitoneal IUDs in asymptomatic 1. Ingec M, Kumtepe Y, Kadanali S, et al. A rare case of ileal embedding
patients is somewhat controversial. The World Health Organization by an intrauterine device. Eur J Contracept Reprod Health Care
2005;10(1):29–31. DOI: 10.1080/13625180500035082.
recommended that displaced IUDs should always be removed to 2. Sharifiaghdas F, Mohammad Ali Beigi F, Abdi H. Laparoscopic removal
prevent possible complications that can occur due to intraperitoneal of a migrated intrauterine device. Urol J 2007;4(3):177–179.
adhesion formation or migration into adjacent organs. 9 3. Meshikhes AW, El-Tair M, Al-Zahir AA. Laparoscopic removal of a
The standard management for a migrated intrauterine migrated intrauterine contraceptive device. J Inst Obstet Gynaecol
contraceptive device (IUCD) is surgical removal, either open 2010;30(3):317–319. DOI: 10.3109/01443610903585200.
or via laparoscopic approach. A review article by Mosley et al. 4. Ohana E, Sheiner E, Leron E, et al. Appendix perforation by an
revealed that majority (93.0%) of reported cases were attempted intrauterine contraceptive device. Eur J Obstet Gynecol Reprod Biol
laparoscopically; however, 22.5% of these were converted to open 2000;88(2):129–131. DOI: 10.1016/S0301-2115(99)00142-6.
7
procedures. The rate of conversion was found to vary according to 5. Zeino MY, Wietfeldt ED, Advani V, et al. Laparoscopic removal
of a copper intrauterine device from the sigmoid colon. JSLS
the site of the displaced IUD. However, it must be noted that their 2011;15(4):568–570. DOI: 10.4293/108680811X13176785204661.
review only included cases in which the IUD was located within 6. Shin DG, Kim TN, Lee W. Intrauterine device embedded into the
the peritoneal cavity; cases with penetration into adjacent organs bladder wall with stone formation: laparoscopic removal is a
88 World Journal of Laparoscopic Surgery, Volume 13 Issue 2 (May–August 2020)