
Page 55 - WJOLS - Journal of Laparoscopic Surgery
P. 55
R Meenakshi Menon
• Bilateral internal iliac artery ligation and dilation and progression toward the bladder is seen. Bladder is dis-
extraction under laparoscopic guidance sected down, and excision of uterine scar is done with
• Selective uterine artery embolization (UAE) + D&C repair of defect in uterus.
and MTX Laparoscopic management is done by local injection of
• Transvaginal resection vasopressin followed by an incision over the bulge after
• Hysteroscopy reflecting the bladder, thereafter enucleating the sac and
A systematic review of the above management options retrieval in an endobag. The uterine incision is sutured.
5
was done by Petersen et al focusing on efficacy and com- Bipolar is used for hemostasis. Some surgeons also make
plications related with each method in 2,037 cases, where
it was found that laparoscopy had 97.1% success rate with a bilateral uterine artery ligation at the start of surgery
7
no severe complications. Rest of the management options to minimize blood loss (Fig. 2).
had a variable success rate. Least success was seen with
expectant management of 41.5% with a complication of ALTERNATIVES
53.7%. Maximum success was noted with high-intensity
focused ultrasound (HIFU) ablation of 100% with no com- Hysteroscopy was also considered an option, but addi-
plications, but only 16 cases were studied as compared tional treatment was required in 17% of cases. Hystero-
with 69 cases who underwent laparoscopy. scopic management of CSP has benefits over local and
Majority of the reviewed articles in this study were systemic MTX with normalization of β-human chorionic
case reports, which was a major limitation in providing gonadotropin level more rapidly and decrease in follow-
conclusions. Also, there was no consensus on individual- up time according to a retrospective cohort study con-
8
izing treatment strategy based on type of CSP or thick- ducted by Deans and Abott in Sydney (Fig. 3).
9
ness of intervening myometrium. 5 In a study done by Pan and Liu, hysteroscopy under
Successful laparoscopic resection of CSP was first laparoscopic guidance was preferred in cases with myome-
reported by Lee et al. 6 trial thickness less than 3 mm to avoid the risk of uterine
perforation and bladder injury. Also, additional advantage
OPERATIVE PROCEDURE
of performing a laparoscopy concomitantly helps in resec-
5
In the review done by Birch Petersen et al, laparoscopy tion and repair in case of perforation of scar site (Table 1
was done under general anesthesia where CSP with and Fig. 4). 10
A B
C D
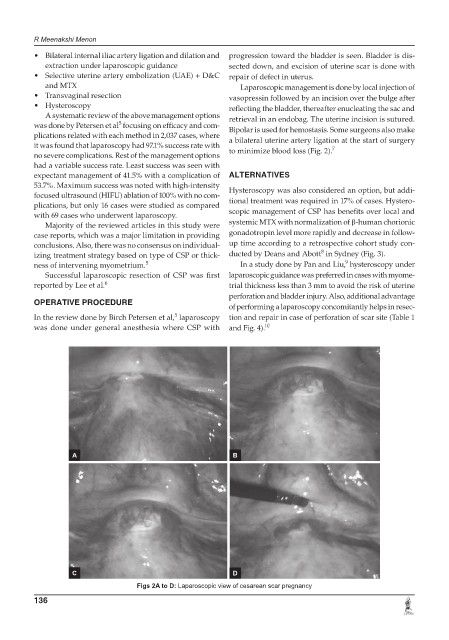
Figs 2A to D: Laparoscopic view of cesarean scar pregnancy
136