
Page 14 - Journal of World Association of Laparoscopic Surgeons
P. 14
Role of Diagnostic Laparoscopy in Chronic Abdominal Pain with Uncertain Diagnosis
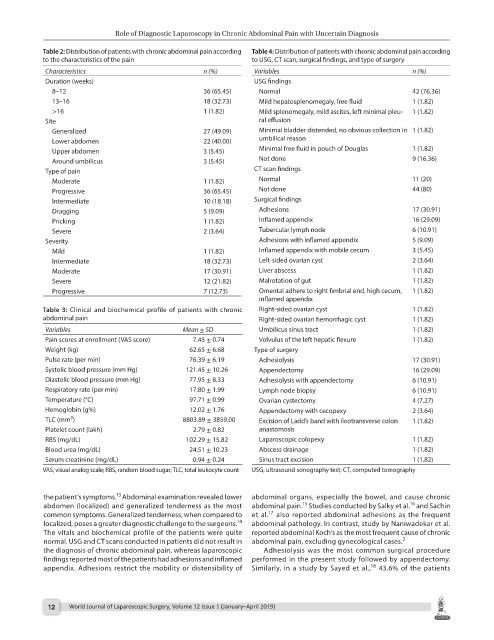
Table 2: Distribution of patients with chronic abdominal pain according Table 4: Distribution of patients with chronic abdominal pain according
to the characteristics of the pain to USG, CT scan, surgical findings, and type of surgery
Characteristics n (%) Variables n (%)
Duration (weeks) USG findings
8–12 36 (65.45) Normal 42 (76.36)
13–16 18 (32.73) Mild hepatosplenomegaly, free fluid 1 (1.82)
>16 1 (1.82) Mild splenomegaly, mild ascites, left minimal pleu- 1 (1.82)
Site ral effusion
Generalized 27 (49.09) Minimal bladder distended, no obvious collection in 1 (1.82)
Lower abdomen 22 (40.00) umbilical reason
Upper abdomen 3 (5.45) Minimal free fluid in pouch of Douglas 1 (1.82)
Around umbilicus 3 (5.45) Not done 9 (16.36)
Type of pain CT scan findings
Moderate 1 (1.82) Normal 11 (20)
Progressive 36 (65.45) Not done 44 (80)
Intermediate 10 (18.18) Surgical findings
Dragging 5 (9.09) Adhesions 17 (30.91)
Pricking 1 (1.82) Inflamed appendix 16 (29.09)
Severe 2 (3.64) Tubercular lymph node 6 (10.91)
Severity Adhesions with inflamed appendix 5 (9.09)
Mild 1 (1.82) Inflamed appendix with mobile cecum 3 (5.45)
Intermediate 18 (32.73) Left-sided ovarian cyst 2 (3.64)
Moderate 17 (30.91) Liver abscess 1 (1.82)
Severe 12 (21.82) Malrotation of gut 1 (1.82)
Progressive 7 (12.73) Omental adhere to right fimbrial end, high cecum, 1 (1.82)
inflamed appendix
Table 3: Clinical and biochemical profile of patients with chronic Right-sided ovarian cyst 1 (1.82)
abdominal pain Right-sided ovarian hemorrhagic cyst 1 (1.82)
Variables Mean ± SD Umbilicus sinus tract 1 (1.82)
Pain scores at enrollment (VAS score) 7.45 ± 0.74 Volvulus of the left hepatic flexure 1 (1.82)
Weight (kg) 62.65 ± 6.68 Type of surgery
Pulse rate (per min) 76.39 ± 6.19 Adhesiolysis 17 (30.91)
Systolic blood pressure (mm Hg) 121.45 ± 10.26 Appendectomy 16 (29.09)
Diastolic blood pressure (mm Hg) 77.95 ± 8.33 Adhesiolysis with appendectomy 6 (10.91)
Respiratory rate (per min) 17.80 ± 1.99 Lymph node biopsy 6 (10.91)
Temperature (°C) 97.71 ± 0.99 Ovarian cystectomy 4 (7.27)
Hemoglobin (g%) 12.02 ± 1.76 Appendectomy with cecopexy 2 (3.64)
3
TLC (mm ) 8803.89 ± 3859.00 Excision of Ladd’s band with ileotransverse colon 1 (1.82)
Platelet count (lakh) 2.79 ± 0.82 anastomosis
RBS (mg/dL) 102.29 ± 15.82 Laparoscopic colopexy 1 (1.82)
Blood urea (mg/dL) 24.51 ± 10.23 Abscess drainage 1 (1.82)
Serum creatinine (mg/dL) 0.94 ± 0.24 Sinus tract excision 1 (1.82)
VAS, visual analog scale; RBS, random blood sugar; TLC, total leukocyte count USG, ultrasound sonography test; CT, computed tomography
13
the patient’s symptoms. Abdominal examination revealed lower abdominal organs, especially the bowel, and cause chronic
16
15
abdomen (localized) and generalized tenderness as the most abdominal pain. Studies conducted by Salky et al. and Sachin
17
common symptoms. Generalized tenderness, when compared to et al. also reported abdominal adhesions as the frequent
14
localized, poses a greater diagnostic challenge to the surgeons. abdominal pathology. In contrast, study by Naniwadekar et al.
The vitals and biochemical profile of the patients were quite reported abdominal Koch’s as the most frequent cause of chronic
2
normal. USG and CT scans conducted in patients did not result in abdominal pain, excluding gynecological cases.
the diagnosis of chronic abdominal pain, whereas laparoscopic Adhesiolysis was the most common surgical procedure
findings reported most of the patients had adhesions and inflamed performed in the present study followed by appendectomy.
18
appendix. Adhesions restrict the mobility or distensibility of Similarly, in a study by Sayed et al., 43.6% of the patients
12 World Journal of Laparoscopic Surgery, Volume 12 Issue 1 (January–April 2019)