
Page 13 - World Journal of Laparoscopic Surgery
P. 13
Total Laparoscopic Hysterectomies at Tertiary Care Center
were inserted 2 inches above and medial to anterior superior iliac Table 1: General characteristics of patients
spine and one central trocar at midpoint of a line between pubic Characteristics Numbers (%)
symphysis and umbilicus, Trocar was inserted one inch lateral
toward left side) After inserting the 10 mm, 30° laparoscope, the Age-group
uterus and adnexal pathologies were identified. Energy source for 30–40 10 (5%)
the surgery consisted of Harmonic scalpel (J & J Ethicon ultrasonic 41–50 182 (91%)
device) and bipolar cautery/shearer/vessel sealer (Alan Indian 51–60 08 (4%)
make). Electro surgical unit (ESU) used was from Alan with bipolar, Parity
monopolar, and vessel sealing function. Vaginal manipulation
was done by a patented specialized Sukhadia manipulator. The 1 13 (6.5%)
main advantage of this manipulator was that it allows anteversion, 2 112 (56%)
retroversion, and side to side movements of uterus and allowed ease More than 2 75 (37.5%)
of access to bilateral uterine arteries; also the vaginal tube made the History of previous surgeries
vault cutting safe and secure by pushing the bladder downward and
ureters laterally. During difficult dissection for bladder and rectum, 0 53 (26.5%)
the dictum followed was fat in the dissecting plane always belongs 1 118 (59%)
to rectum and bladder. 2 21 (10.5%)
More than 2 8 (4%)
surgIcAl steps
Right round ligament, ovarian ligament and fallopian tube Table 2: Clinical characteristics of patients
were coagulated and cut if ovaries are to be conserved. Characteristics Numbers (%)
Infundibulopelvic ligament were coagulated and cut in cases of Presenting symptoms
associated ovarian pathologies. Similar procedure repeated on Heavy menstrual bleeding 151 (75.5%)*
the left side. Separation of the bladder was done with the help of
harmonic scalpel and uterovesical fold and bladder were pushed Pain in the abdomen 131 (65.5%)*
down. Posterior peritoneum was dissected down and ureters were White discharge per vaginum 43 (21.5%)
identified. In cases with advanced bladder or bladder adhesion Lump in the abdomen 10 (5%)
[in cases of previous 1 or more lower segment caesarean section Inter-menstrual bleeding 12 (6%)
(LSCS)] sharp dissection was done and bladder dissection is done Uterine size
through the lateral window technique. The vaginal manipulation
helped and facilitated the bladder dissection by traction and Normal 09 (4.5%)
counter traction technique. In difficult cases where cervix is pulled Bulky 81 (40.5%)
up due to previous multiple caesarean surgeries/cervical fibroid/ 6–12 weeks 88 (44%)
pelvic surgeries/advanced endometriosis, myoma screw was used 12–16 weeks 22 (11%)
for uterine manipulation. Bilateral uterine arteries were identified *Since the patients had multiple complaints, thus the aggregate is more
at the level of isthmus, coagulated, and cut. Hemostasis was than 100%
confirmed. Bilateral uterosacral ligament was coagulated and cut
using harmonics. Vault was cut by giving circumferential incision
over the vaginal manipulator. Specimen was delivered out by
vaginal route. Wherever necessary, the manual morcellation was
carried out vaginally. Vaginal vault was sutured by vicryl round
body no 1 by continuous interlocking intracorporeal suturing
technique. Bladder, bowel, and hemostasis were checked. All
accessories port were removed under vision. Carbon dioxide
(CO ) desufflation was done. Main port was removed. Port sites
2
were sutured with ethilon 2-0/stainless steel clip. Sterile dressing
was done. Patient’s postoperative course was monitored. Patient
catheter was removed on day 2, oral started after 8 hours. Patient
discharged on day 3 and follow-up on day 7 and day 21.
results
The demographic characteristics of the patients who underwent
TLH at our study center include (1) the mean age of the patient in the
study was 42 years; (2) parity in the majority (56%) was 2, while 59%
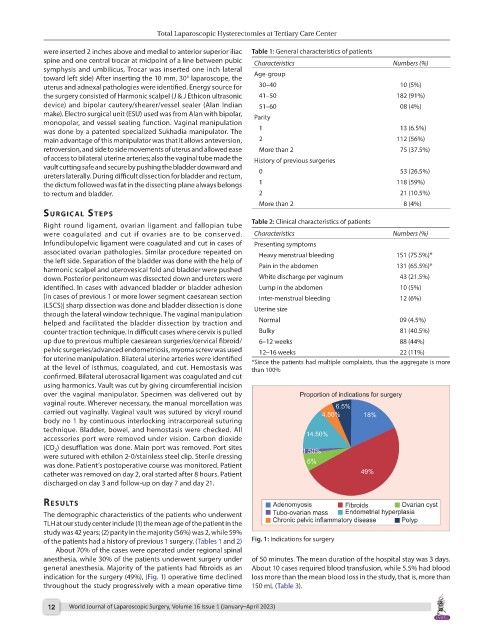
of the patients had a history of previous 1 surgery. (Tables 1 and 2) Fig. 1: Indications for surgery
About 70% of the cases were operated under regional spinal
anesthesia, while 30% of the patients underwent surgery under of 50 minutes. The mean duration of the hospital stay was 3 days.
general anesthesia. Majority of the patients had fibroids as an About 10 cases required blood transfusion, while 5.5% had blood
indication for the surgery (49%), (Fig. 1) operative time declined loss more than the mean blood loss in the study, that is, more than
throughout the study progressively with a mean operative time 150 mL (Table 3).
12 World Journal of Laparoscopic Surgery, Volume 16 Issue 1 (January–April 2023)