
Page 5 - World Journal of Laparoscopic Surgery
P. 5
First Port Access Using an Optical Trocar
dIscussIon
Our study shows that the given technique for gaining access into
the abdominal cavity using the optical trocar with 0°-degree
camera adds advantages over the conventional blind method using
Veress needle and also the open technique. It allows a completely
safe and fast method for insufflation and first port access under
complete direct vision. This technique may be used as well in re-do
operations and patients having previous surgeries, but still great
care during access is required to avoid complications. The point
of entry described in our technique needed to be well recognized
to allow to get the benefits of avoiding vascular or organ injury
and easy manipulation of the instruments during carrying out
the procedure required; otherwise, it might add more burden
during the operation. The incidence of postoperative hernia in our
technique was zero compared to other techniques especially the
open one which had higher incidence rates because of introduction
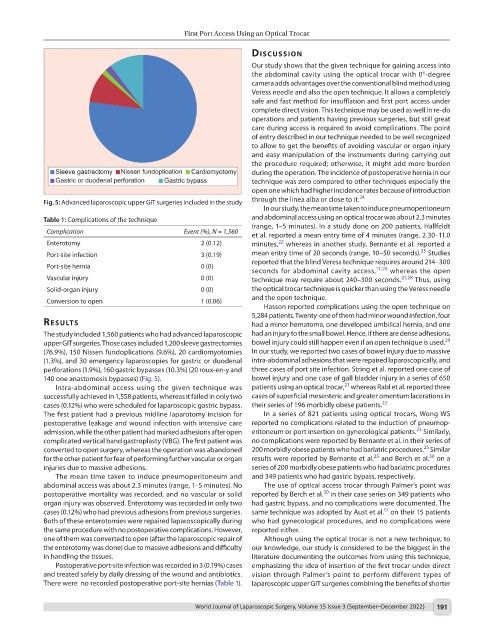
Fig. 5: Advanced laparoscopic upper GIT surgeries included in the study through the linea alba or close to it. 24
In our study, the mean time taken to induce pneumoperitoneum
Table 1: Complications of the technique and abdominal access using an optical trocar was about 2.3 minutes
(range, 1–5 minutes). In a study done on 200 patients, Hallfeldt
Complication Event (%), N = 1,560
et al. reported a mean entry time of 4 minutes (range, 2.30–11.0
22
Enterotomy 2 (0.12) minutes, whereas in another study, Bernante et al. reported a
25
Port-site infection 3 (0.19) mean entry time of 20 seconds (range, 10–50 seconds). Studies
reported that the blind Veress technique requires around 214–300
Port-site hernia 0 (0) 11,26
seconds for abdominal cavity access, whereas the open
Vascular injury 0 (0) technique may require about 240–300 seconds. 27,28 Thus, using
Solid-organ injury 0 (0) the optical trocar technique is quicker than using the Veress needle
Conversion to open 1 (0.06) and the open technique.
Hasson reported complications using the open technique on
5,284 patients. Twenty-one of them had minor wound infection, four
results had a minor hematoma, one developed umbilical hernia, and one
The study included 1,560 patients who had advanced laparoscopic had an injury to the small bowel. Hence, if there are dense adhesions,
29
upper GIT surgeries. Those cases included 1,200 sleeve gastrectomies bowel injury could still happen even if an open technique is used.
(76.9%), 150 Nissen fundoplications (9.6%), 20 cardiomyotomies In our study, we reported two cases of bowel injury due to massive
(1.3%), and 30 emergency laparoscopies for gastric or duodenal intra-abdominal adhesions that were repaired laparoscopically, and
perforations (1.9%), 160 gastric bypasses (10.3%) (20 roux-en-y and three cases of port site infection. String et al. reported one case of
140 one anastomosis bypasses) (Fig. 5). bowel injury and one case of gall bladder injury in a series of 650
21
Intra-abdominal access using the given technique was patients using an optical trocar, whereas Rabl et al. reported three
successfully achieved in 1,558 patients, whereas it failed in only two cases of superficial mesenteric and greater omentum lacerations in
cases (0.12%) who were scheduled for laparoscopic gastric bypass. their series of 196 morbidly obese patients. 22
The first patient had a previous midline laparotomy incision for In a series of 821 patients using optical trocars, Wong WS
postoperative leakage and wound infection with intensive care reported no complications related to the induction of pneumop-
23
admission, while the other patient had marked adhesions after open eritoneum or port insertion on gynecological patients. Similarly,
complicated vertical band gastroplasty (VBG). The first patient was no complications were reported by Bernante et al. in their series of
25
converted to open surgery, whereas the operation was abandoned 200 morbidly obese patients who had bariatric procedures. Similar
30
25
for the other patient for fear of performing further vascular or organ results were reported by Bernante et al. and Berch et al. on a
injuries due to massive adhesions. series of 200 morbidly obese patients who had bariatric procedures
The mean time taken to induce pneumoperitoneum and and 349 patients who had gastric bypass, respectively.
abdominal access was about 2.3 minutes (range, 1–5 minutes). No The use of optical access trocar through Palmer’s point was
30
postoperative mortality was recorded, and no vascular or solid reported by Berch et al. in their case series on 349 patients who
organ injury was observed. Enterotomy was recorded in only two had gastric bypass, and no complications were documented. The
17
cases (0.12%) who had previous adhesions from previous surgeries. same technique was adopted by Aust et al. on their 15 patients
Both of these enterotomies were repaired laparoscopically during who had gynecological procedures, and no complications were
the same procedure with no postoperative complications. However, reported either.
one of them was converted to open (after the laparoscopic repair of Although using the optical trocar is not a new technique, to
the enterotomy was done) due to massive adhesions and difficulty our knowledge, our study is considered to be the biggest in the
in handling the tissues. literature documenting the outcomes from using this technique,
Postoperative port-site infection was recorded in 3 (0.19%) cases emphasizing the idea of insertion of the first trocar under direct
and treated safely by daily dressing of the wound and antibiotics. vision through Palmer’s point to perform different types of
There were no recorded postoperative port-site hernias (Table 1). laparoscopic upper GIT surgeries combining the benefits of shorter
World Journal of Laparoscopic Surgery, Volume 15 Issue 3 (September–December 2022) 191