
Page 4 - World Journal of Laparoscopic Surgery
P. 4
First Port Access Using an Optical Trocar
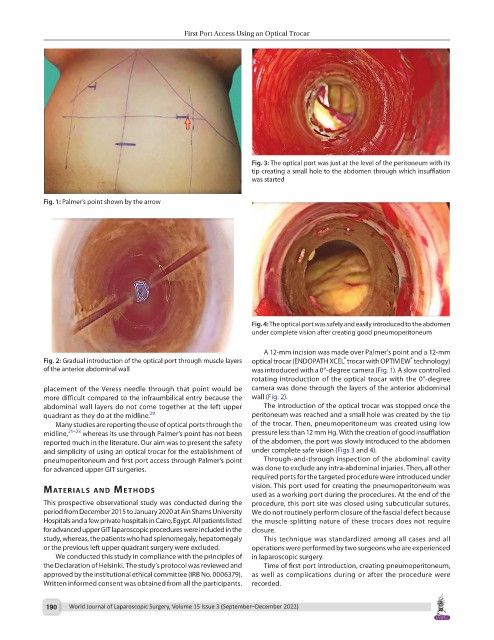
Fig. 3: The optical port was just at the level of the peritoneum with its
tip creating a small hole to the abdomen through which insufflation
was started
Fig. 1: Palmer’s point shown by the arrow
Fig. 4: The optical port was safely and easily introduced to the abdomen
under complete vision after creating good pneumoperitoneum
A 12-mm incision was made over Palmer’s point and a 12-mm
®
®
Fig. 2: Gradual introduction of the optical port through muscle layers optical trocar (ENDOPATH XCEL trocar with OPTIVIEW technology)
of the anterior abdominal wall was introduced with a 0°-degree camera (Fig. 1). A slow controlled
rotating introduction of the optical trocar with the 0°-degree
placement of the Veress needle through that point would be camera was done through the layers of the anterior abdominal
more difficult compared to the infraumbilical entry because the wall (Fig. 2).
abdominal wall layers do not come together at the left upper The introduction of the optical trocar was stopped once the
quadrant as they do at the midline. 20 peritoneum was reached and a small hole was created by the tip
Many studies are reporting the use of optical ports through the of the trocar. Then, pneumoperitoneum was created using low
midline, 21–23 whereas its use through Palmer’s point has not been pressure less than 12 mm Hg. With the creation of good insufflation
reported much in the literature. Our aim was to present the safety of the abdomen, the port was slowly introduced to the abdomen
and simplicity of using an optical trocar for the establishment of under complete safe vision (Figs 3 and 4).
pneumoperitoneum and first port access through Palmer’s point Through-and-through inspection of the abdominal cavity
for advanced upper GIT surgeries. was done to exclude any intra-abdominal injuries. Then, all other
required ports for the targeted procedure were introduced under
vision. This port used for creating the pneumoperitoneum was
MAterIAls And Methods
used as a working port during the procedures. At the end of the
This prospective observational study was conducted during the procedure, this port site was closed using subcuticular sutures.
period from December 2015 to January 2020 at Ain Shams University We do not routinely perform closure of the fascial defect because
Hospitals and a few private hospitals in Cairo, Egypt. All patients listed the muscle-splitting nature of these trocars does not require
for advanced upper GIT laparoscopic procedures were included in the closure.
study, whereas, the patients who had splenomegaly, hepatomegaly This technique was standardized among all cases and all
or the previous left upper quadrant surgery were excluded. operations were performed by two surgeons who are experienced
We conducted this study in compliance with the principles of in laparoscopic surgery.
the Declaration of Helsinki. The study’s protocol was reviewed and Time of first port introduction, creating pneumoperitoneum,
approved by the institutional ethical committee (IRB No. 0006379). as well as complications during or after the procedure were
Written informed consent was obtained from all the participants. recorded.
190 World Journal of Laparoscopic Surgery, Volume 15 Issue 3 (September–December 2022)