
Page 56 - tmp
P. 56
Laparoscopic TEP Using 3D Mesh to Treat Bilateral Inguinal Hernia
patients having a laparoscopic appendectomy (4.0%), one patient hole was mainly from 1.5 to 3 cm with 84.0%. There were 82.0% of
having cholecystectomy (2.0%), and one patient having open patients using small 3D mesh (8.5 × 13.7 cm) and one case required
2
appendectomy (2.0%). The average BMI was 21.3 ± 2.6 kg/m (Table 1). mesh fixation (2.0%). Seven patients (14.0%) had complications during
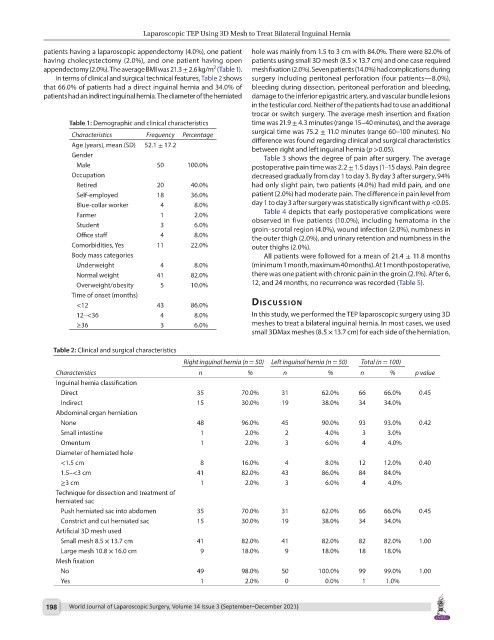
In terms of clinical and surgical technical features, Table 2 shows surgery including peritoneal perforation (four patients—8.0%),
that 66.0% of patients had a direct inguinal hernia and 34.0% of bleeding during dissection, peritoneal perforation and bleeding,
patients had an indirect inguinal hernia. The diameter of the herniated damage to the inferior epigastric artery, and vascular bundle lesions
in the testicular cord. Neither of the patients had to use an additional
trocar or switch surgery. The average mesh insertion and fixation
Table 1: Demographic and clinical characteristics time was 21.9 ± 4.3 minutes (range 15–40 minutes), and the average
surgical time was 75.2 ± 11.0 minutes (range 60–100 minutes). No
Characteristics Frequency Percentage difference was found regarding clinical and surgical characteristics
Age (years), mean (SD) 52.1 ± 17.2 between right and left inguinal hernia (p >0.05).
Gender Table 3 shows the degree of pain after surgery. The average
Male 50 100.0% postoperative pain time was 2.2 ± 1.5 days (1–15 days). Pain degree
Occupation decreased gradually from day 1 to day 3. By day 3 after surgery, 94%
Retired 20 40.0% had only slight pain, two patients (4.0%) had mild pain, and one
Self-employed 18 36.0% patient (2.0%) had moderate pain. The difference in pain level from
Blue-collar worker 4 8.0% day 1 to day 3 after surgery was statistically significant with p <0.05.
Table 4 depicts that early postoperative complications were
Farmer 1 2.0% observed in five patients (10.0%), including hematoma in the
Student 3 6.0% groin–scrotal region (4.0%), wound infection (2.0%), numbness in
Office staff 4 8.0% the outer thigh (2.0%), and urinary retention and numbness in the
Comorbidities, Yes 11 22.0% outer thighs (2.0%).
Body mass categories All patients were followed for a mean of 21.4 ± 11.8 months
Underweight 4 8.0% (minimum 1 month, maximum 40 months). At 1 month postoperative,
Normal weight 41 82.0% there was one patient with chronic pain in the groin (2.1%). After 6,
Overweight/obesity 5 10.0% 12, and 24 months, no recurrence was recorded (Table 5).
Time of onset (months)
<12 43 86.0% dIscussIon
12–<36 4 8.0% In this study, we performed the TEP laparoscopic surgery using 3D
≥36 3 6.0% meshes to treat a bilateral inguinal hernia. In most cases, we used
small 3DMax meshes (8.5 × 13.7 cm) for each side of the herniation.
Table 2: Clinical and surgical characteristics
Right inguinal hernia (n = 50) Left inguinal hernia (n = 50) Total (n = 100)
Characteristics n % n % n % p value
Inguinal hernia classification
Direct 35 70.0% 31 62.0% 66 66.0% 0.45
Indirect 15 30.0% 19 38.0% 34 34.0%
Abdominal organ herniation
None 48 96.0% 45 90.0% 93 93.0% 0.42
Small intestine 1 2.0% 2 4.0% 3 3.0%
Omentum 1 2.0% 3 6.0% 4 4.0%
Diameter of herniated hole
<1.5 cm 8 16.0% 4 8.0% 12 12.0% 0.40
1.5–<3 cm 41 82.0% 43 86.0% 84 84.0%
≥3 cm 1 2.0% 3 6.0% 4 4.0%
Technique for dissection and treatment of
herniated sac
Push herniated sac into abdomen 35 70.0% 31 62.0% 66 66.0% 0.45
Constrict and cut herniated sac 15 30.0% 19 38.0% 34 34.0%
Artificial 3D mesh used
Small mesh 8.5 × 13.7 cm 41 82.0% 41 82.0% 82 82.0% 1.00
Large mesh 10.8 × 16.0 cm 9 18.0% 9 18.0% 18 18.0%
Mesh fixation
No 49 98.0% 50 100.0% 99 99.0% 1.00
Yes 1 2.0% 0 0.0% 1 1.0%
198 World Journal of Laparoscopic Surgery, Volume 14 Issue 3 (September–December 2021)