
Page 36 - WJOLS - Laparoscopic Journal
P. 36
Thawatchai Tullavardhana
costal margin and the iliac crest (Figs 3A and B). This 3. Left adrenal vein are located at inferomedial of adrenal
position is most widely used because it permits proper bowel gland in conjunction with left renal vein. Identification
mobilization and makes exposure of the surgical area. of left adrenal vein at this level then clipped and divided.
Retroperitoneal space access: Open Hasson’s technique by 4. Continue mobilization thought lateral and inferior surfaces
made 2 cm skin incision is at 2 cm below the inferior edge of adrenal gland and carefully dissected away from the
of the twelfth rib then split the muscles until the lumbodorsal kidney. Then superior aspect and inferior phrenic vessels
fascia was divided by blunt dissection then enter to are controlled with ultrasonic laparoscopic coagulation
retroperitoneal space. Retroperitoneal requires the creation instrument or bipolar cautery.
of a working space using a balloon dilatation (800 cc of air 5. Adrenal gland was extracted in a sterile plastic bag and
inflated to balloon). extracted from primary port. The trocars were removed
Port site placement: After dilatation, 10 mm trocar was and suture skin incision.
inserted for 30 degree 10 mm laparoscope, then insufflations
of carbon dioxide to generate pneumoretroperitoneum Right Adrenalectomy
pressure of 15 mm Hg. A second trocar is placed in the
anterior axillary line midway between the costal margin and 1. Dissection of right adrenal gland is the same principle
iliac crest. A third port is placed posteriorly between the of left adrenal gland dissection. Psoas muscle is the
twelfth rib and iliac crest along the lateral border of the important key anatomical landmark.
sacrospinalis muscle. A fourth port (5 mm) is inserted for 2. After identification of right kidney and right adrenal gland.
retraction of the kidney and is placed cephalad to the first Carefully dissection of IVC that is located at medial part
port in the anterior axillary line. An optional fourth port is of psoas muscle.
placed in the anterior axillary line 5 to 7 cm inferior to the 3. Right adrenal vein was identified in conjunction of IVC
third port and may be used for retraction during dissection the clipped and divided. Avoiding of avulsion injury that
of adrenal gland. may be causing massive hemorrhage.
4. After completion of adrenal gland dissection, specimen
Operative Approach 3-5,7 was extracted in a sterile plastic bag and extracted from
Important key anatomical landmark of this surgical approach primary port. The trocars were removed and suture skin
is psoas muscle. The kidney and adrenal gland locate on incision.
lateral border.
Posterior Retroperitoneal Approach
Left Adrenalectomy This technique was initially reported in 1999 by Walz et al.
1. Dissection along lateral border of psoas muscle to medial The patient is placed on a lateral flank technique and creation
border left kidney, then retract kidney upward and of working space by balloon dilatation as described in lateral
anteriorly. retroperitoneal approach. A three- to four-port was used
2. Carefully dissection of renal hilum to identified left renal for camera and working instruments. Initial dissection was
vein and medial border of adrenal gland. performed at superior of adrenal gland continue thought
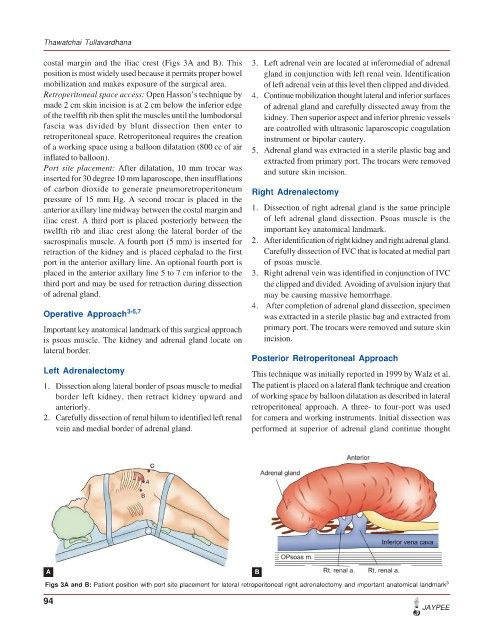
A B
Figs 3A and B: Patient position with port site placement for lateral retroperitoneal right adrenalectomy and important anatomical landmark 3
94
JAYPEE