
Page 31 - WJOLS - Laparoscopic Journal
P. 31
Review of Literatures on Laparoscopic Prosthetic Repair of Giant Hiatal Hernia than Pure Anatomical Repair of Crura
Acellular human dermal matrix may be an effective
method to buttress the crural closure in patients with large
hiatal hernias. Longer follow-up in larger numbers of patients
is needed to assess the validity of this approach. 25
COMPLICATIONS
Early nonreoperative complications 26
• Dysphagia
• Heartburn
• Chest pain
• Fever
• Epigastric pain
• Weight loss.
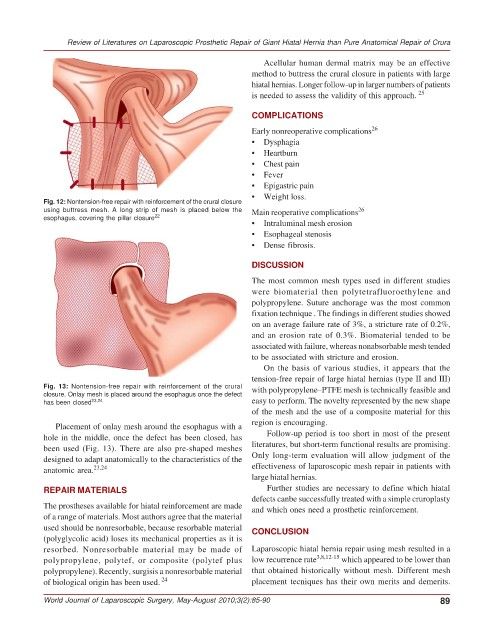
Fig. 12: Nontension-free repair with reinforcement of the crural closure
using buttress mesh. A long strip of mesh is placed below the Main reoperative complications 26
esophagus, covering the pillar closure 22
• Intraluminal mesh erosion
• Esophageal stenosis
• Dense fibrosis.
DISCUSSION
The most common mesh types used in different studies
were biomaterial then polytetrafluoroethylene and
polypropylene. Suture anchorage was the most common
fixation technique . The findings in different studies showed
on an average failure rate of 3%, a stricture rate of 0.2%,
and an erosion rate of 0.3%. Biomaterial tended to be
associated with failure, whereas nonabsorbable mesh tended
to be associated with stricture and erosion.
On the basis of various studies, it appears that the
tension-free repair of large hiatal hernias (type II and III)
Fig. 13: Nontension-free repair with reinforcement of the crural with polypropylene–PTFE mesh is technically feasible and
closure. Onlay mesh is placed around the esophagus once the defect
has been closed 23,24 easy to perform. The novelty represented by the new shape
of the mesh and the use of a composite material for this
region is encouraging.
Placement of onlay mesh around the esophagus with a
hole in the middle, once the defect has been closed, has Follow-up period is too short in most of the present
been used (Fig. 13). There are also pre-shaped meshes literatures, but short-term functional results are promising.
designed to adapt anatomically to the characteristics of the Only long-term evaluation will allow judgment of the
anatomic area. 23,24 effectiveness of laparoscopic mesh repair in patients with
large hiatal hernias.
REPAIR MATERIALS Further studies are necessary to define which hiatal
defects canbe successfully treated with a simple cruroplasty
The prostheses available for hiatal reinforcement are made and which ones need a prosthetic reinforcement.
of a range of materials. Most authors agree that the material
used should be nonresorbable, because resorbable material CONCLUSION
(polyglycolic acid) loses its mechanical properties as it is
resorbed. Nonresorbable material may be made of Laparoscopic hiatal hernia repair using mesh resulted in a
polypropylene, polytef, or composite (polytef plus low recurrence rate 3,8,12-15 which appeared to be lower than
polypropylene). Recently, surgisis a nonresorbable material that obtained historically without mesh. Different mesh
of biological origin has been used. 24 placement tecniques has their own merits and demerits.
World Journal of Laparoscopic Surgery, May-August 2010;3(2):85-90 89