
Page 35 - WJOLS - Laparoscopic Journal
P. 35
Laparoscopic Adrenalectomy: Surgical Technique
A B
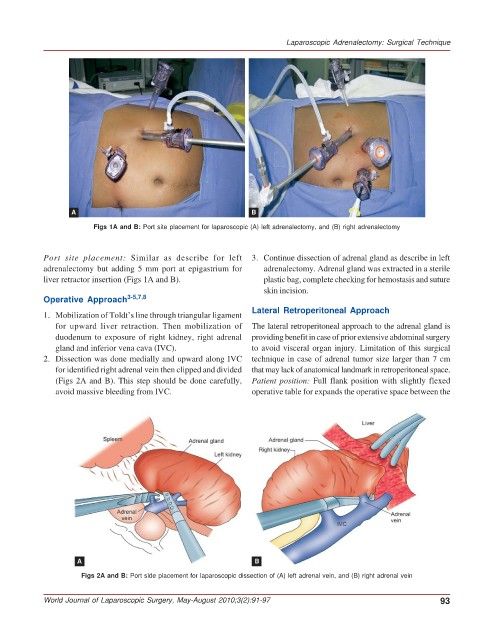
Figs 1A and B: Port site placement for laparoscopic (A) left adrenalectomy, and (B) right adrenalectomy
Port site placement: Similar as describe for left 3. Continue dissection of adrenal gland as describe in left
adrenalectomy but adding 5 mm port at epigastrium for adrenalectomy. Adrenal gland was extracted in a sterile
liver retractor insertion (Figs 1A and B). plastic bag, complete checking for hemostasis and suture
skin incision.
Operative Approach 3-5,7,8
Lateral Retroperitoneal Approach
1. Mobilization of Toldt’s line through triangular ligament
for upward liver retraction. Then mobilization of The lateral retroperitoneal approach to the adrenal gland is
duodenum to exposure of right kidney, right adrenal providing benefit in case of prior extensive abdominal surgery
gland and inferior vena cava (IVC). to avoid visceral organ injury. Limitation of this surgical
2. Dissection was done medially and upward along IVC technique in case of adrenal tumor size larger than 7 cm
for identified right adrenal vein then clipped and divided that may lack of anatomical landmark in retroperitoneal space.
(Figs 2A and B). This step should be done carefully, Patient position: Full flank position with slightly flexed
avoid massive bleeding from IVC. operative table for expands the operative space between the
A B
Figs 2A and B: Port side placement for laparoscopic dissection of (A) left adrenal vein, and (B) right adrenal vein
World Journal of Laparoscopic Surgery, May-August 2010;3(2):91-97 93