
Page 45 - World Journal of Laparoscopic Surgery
P. 45
Single-port Splenectomy for a Cyst with High CA 19-9
discussion They are usually asymptomatic, but when they are large,
Splenic cysts are rare diseases, with an estimated incidence of as in our patient, can produce symptoms such as abdominal
0.07%. The incidence is higher in young women between 18 years pain, postprandial discomfort due to compression of the
and 46 years. stomach, sensation of a palpable mass, hemorrhage, infection or
2
They are classified as parasitic and nonparasitic. The nonparasitic spontaneous rupture.
are subdivided into true or primary cysts (25%) and pseudocysts or The diagnosis is usually done with imaging tests: Abdominal
secondary cysts (75%) depending on the presence of a coating of ultrasound shows the cystic lesion that may have septa inside; CT
epithelial cells inside the cyst. 1 scan can show calcifications in the cystic wall; the NMR reveals
3
a hyperintensity signal in the T1 and T2 sequences. In addition,
11% of cases are diagnosed when a complication occurs, such as
bleeding, rupture, and infection.
CA 19-9 is a glycoprotein produced in the epithelial cells of the
ducts of the salivary glands, pancreatic duct, bile, and metaplastic
mesothelial cells. It can be elevated in gastrointestinal, pancreatic,
and biliary carcinomas, so it is used as a tumor marker, although
we can find false positives in benign diseases such as cholangitis,
pancreatitis, liver cirrhosis, cystic fibrosis, and idiopathic pulmonary
fibrosis. 4
An increase in CA 19-9 level does not indicate malignancy in
this type of cystic tumors, although the surgeon must be alert
to dismiss the possibility of a cystic pancreatic tumor. There are
similar cases reported in the literature with a CA 19-9 blood level
normalized after splenectomy and the anatomopathological
5
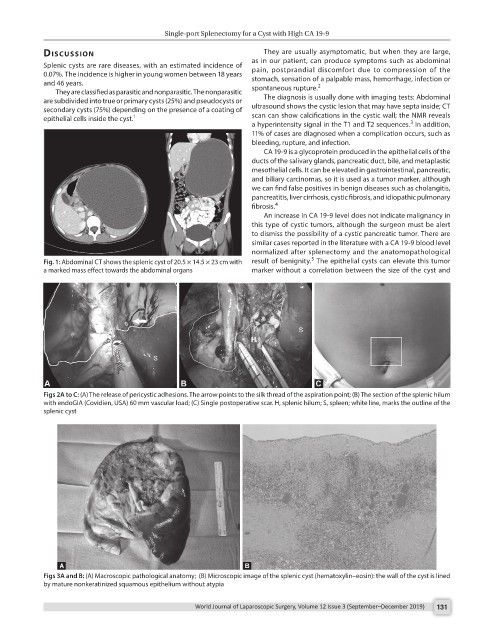
Fig. 1: Abdominal CT shows the splenic cyst of 20.5 × 14.5 × 23 cm with result of benignity. The epithelial cysts can elevate this tumor
a marked mass effect towards the abdominal organs marker without a correlation between the size of the cyst and
Figs 2A to C: (A) The release of pericystic adhesions. The arrow points to the silk thread of the aspiration point; (B) The section of the splenic hilum
with endoGIA (Covidien, USA) 60 mm vascular load; (C) Single postoperative scar. H, splenic hilum; S, spleen; white line, marks the outline of the
splenic cyst
Figs 3A and B: (A) Macroscopic pathological anatomy; (B) Microscopic image of the splenic cyst (hematoxylin–eosin): the wall of the cyst is lined
by mature nonkeratinized squamous epithelium without atypia
World Journal of Laparoscopic Surgery, Volume 12 Issue 3 (September–December 2019) 131