
Page 36 - WJOLS - Laparoscopic Journal
P. 36
Sanjeev Kumar Sareen
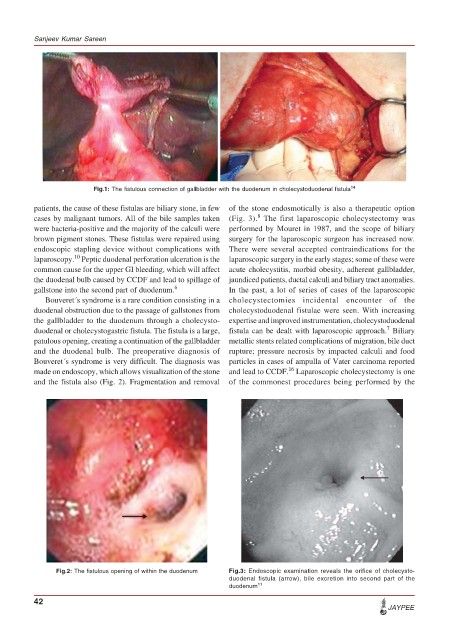
Fig.1: The fistulous connection of gallbladder with the duodenum in cholecystoduodenal fistula 14
patients, the cause of these fistulas are biliary stone, in few of the stone endosmotically is also a therapeutic option
8
cases by malignant tumors. All of the bile samples taken (Fig. 3). The first laparoscopic cholecystectomy was
were bacteria-positive and the majority of the calculi were performed by Mouret in 1987, and the scope of biliary
brown pigment stones. These fistulas were repaired using surgery for the laparoscopic surgeon has increased now.
endoscopic stapling device without complications with There were several accepted contraindications for the
10
laparoscopy. Peptic duodenal perforation ulceration is the laparoscopic surgery in the early stages; some of these were
common cause for the upper GI bleeding, which will affect acute cholecystitis, morbid obesity, adherent gallbladder,
the duodenal bulb caused by CCDF and lead to spillage of jaundiced patients, ductal calculi and biliary tract anomalies.
gallstone into the second part of duodenum. 6 In the past, a lot of series of cases of the laparoscopic
Bouveret´s syndrome is a rare condition consisting in a cholecystectomies incidental encounter of the
duodenal obstruction due to the passage of gallstones from cholecystoduodenal fistulae were seen. With increasing
the gallbladder to the duodenum through a cholecysto- expertise and improved instrumentation, cholecystoduodenal
7
duodenal or cholecystogastric fistula. The fistula is a large, fistula can be dealt with laparoscopic approach. Biliary
patulous opening, creating a continuation of the gallbladder metallic stents related complications of migration, bile duct
and the duodenal bulb. The preoperative diagnosis of rupture; pressure necrosis by impacted calculi and food
Bouveret´s syndrome is very difficult. The diagnosis was particles in cases of ampulla of Vater carcinoma reported
16
made on endoscopy, which allows visualization of the stone and lead to CCDF. Laparoscopic cholecystectomy is one
and the fistula also (Fig. 2). Fragmentation and removal of the commonest procedures being performed by the
Fig.2: The fistulous opening of within the duodenum Fig.3: Endoscopic examination reveals the orifice of cholecysto-
duodenal fistula (arrow), bile excretion into second part of the
duodenum 11
42
JAYPEE