
Page 33 - Peer Reviewed Laparoscopic Jornal
P. 33
WJOLS
Hysteroscopic Findings in an Unusual Case of Adenomyosis
POD was completely obliterated with dense bowel adhesions. McCauseland et al postulated that myometrial hyper-
1
Right ovary was normal. Left ovary was buried in POD. trophy is caused by the ectopic endometrial glands. This
Final diagnosis was adenomyosis with stage IV endometriosis. dysfunctional myometrium is inefficient in contracting and
Considering the wish for fertility, she was put on injection tamponading the bleeding myometrial arterioles. Brosens
Lupron depot for 3 months and planned for IVF subsequently. showed that widened junctional zone has reduction in
peristalsis compared to normal menstruating subendometrial
DISCUSSION zone and results in the menorrhagia. 2
Adenomyosis usually presents as dysmenorrhea, menorrhagia In this case, the patient was referred as a case of fibroid
and chronic pelvic pain in multiparous women in the fourth uterus.
or fifth decade of life. Transvaginal ultrasound has a sensitivity, specificity,
The diagnosis was traditionally histopathological with positive and negative predictive values of 76.4, 92.8, 73.8
hysterectomy specimens. With availability of imaging and 88.8% respectively, in the diagnosis of adenomyosis.
modalities, more and more cases are being diagnosed with Typical ultrasound features of adenomyosis differentiating
transvaginal ultrasound and color Doppler and magnetic it from fibroid uterus are described. 3
resonance ultrasound. The features that differentiate it from fibroid are echo
Also, atypical presentations are coming to the fore. In texture which is not uniform, with poorly defined borders,
this patient, the disease presented early at the age of minimal mass effect on the endometrium or the serosa
23 years. We could not find any similar report in the relative to the size of the lesion, elliptical rather than globular
literature of early presentation of adenomyosis. Menorrhagia shape, lack of edge shadowing; ‘shaggy’ or whorled
was the presenting complaint in this case. All other causes appearance of the endometrium, small myometrial cysts or
of excessive bleeding were ruled out. spaces scattered throughout the myometrium, echogenic
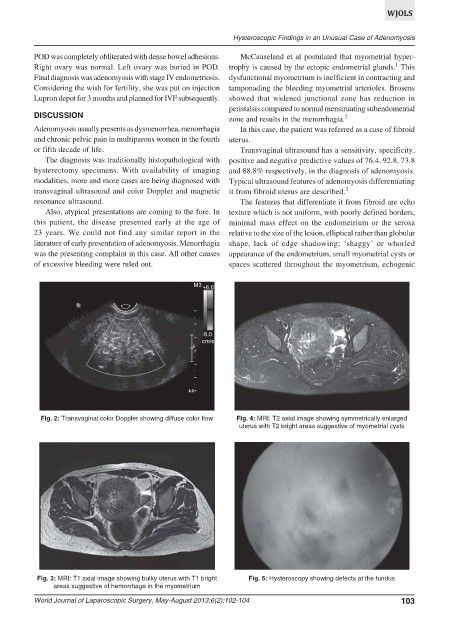
Fig. 2: Transvaginal color Doppler showing diffuse color flow Fig. 4: MRI: T2 axial image showing symmetrically enlarged
uterus with T2 bright areas suggestive of myometrial cysts
Fig. 3: MRI: T1 axial image showing bulky uterus with T1 bright Fig. 5: Hysteroscopy showing defects at the fundus
areas suggestive of hemorrhage in the myometrium
World Journal of Laparoscopic Surgery, May-August 2013;6(2):102-104 103