
Page 34 - Peer Reviewed Laparoscopic Jornal
P. 34
Priya Bhave Chittawar et al
An office hysteroscopy has emerged as one of the
primary investigations in cases of abnormal uterine bleeding
and infertility. If the diagnosis of adenomyosis is not kept
in mind, the appearance of circular endometrial defects can
be confused with intrauterine adhesions leading to
unnecessary operative intervention. Such a picture has been
reported only once but is probably under-reported due to
low awareness among clinicians.
Awareness of the hysteroscopic picture can aid clinicians
in clinching the diagnosis of adenomyosis early thereby
tailoring the treatment according to the symptoms and
conditions.
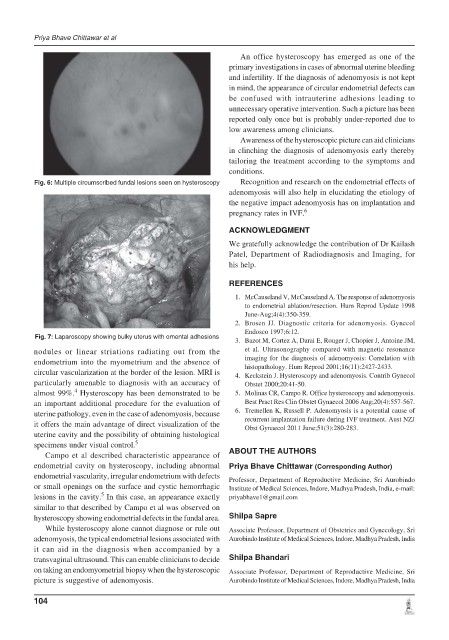
Fig. 6: Multiple circumscribed fundal lesions seen on hysteroscopy Recognition and research on the endometrial effects of
adenomyosis will also help in elucidating the etiology of
the negative impact adenomyosis has on implantation and
pregnancy rates in IVF. 6
ACKNOWLEDGMENT
We gratefully acknowledge the contribution of Dr Kailash
Patel, Department of Radiodiagnosis and Imaging, for
his help.
REFERENCES
1. McCauseland V, McCauseland A. The response of adenomyosis
to endometrial ablation/resection. Hum Reprod Update 1998
June-Aug;4(4):350-359.
2. Brosen JJ. Diagnostic criteria for adenomyosis. Gynecol
Endosco 1997;6:12.
Fig. 7: Laparoscopy showing bulky uterus with omental adhesions
3. Bazot M, Cortez A, Darai E, Rouger J, Chopier J, Antoine JM,
nodules or linear striations radiating out from the et al. Ultrasonography compared with magnetic resonance
endometrium into the myometrium and the absence of imaging for the diagnosis of adenomyosis: Correlation with
histopathology. Hum Reprod 2001;16(11):2427-2433.
circular vascularization at the border of the lesion. MRI is 4. Keckstein J. Hysteroscopy and adenomyosis. Contrib Gynecol
particularly amenable to diagnosis with an accuracy of Obstet 2000;20:41-50.
4
almost 99%. Hysteroscopy has been demonstrated to be 5. Molinas CR, Campo R. Office hysteroscopy and adenomyosis.
an important additional procedure for the evaluation of Best Pract Res Clin Obstet Gynaecol 2006 Aug;20(4):557-567.
uterine pathology, even in the case of adenomyosis, because 6. Tremellen K, Russell P. Adenomyosis is a potential cause of
it offers the main advantage of direct visualization of the recurrent implantation failure during IVF treatment. Aust NZJ
Obst Gynaecol 2011 June;51(3):280-283.
uterine cavity and the possibility of obtaining histological
specimens under visual control. 5
Campo et al described characteristic appearance of ABOUT THE AUTHORS
endometrial cavity on hysteroscopy, including abnormal Priya Bhave Chittawar (Corresponding Author)
endometrial vascularity, irregular endometrium with defects Professor, Department of Reproductive Medicine, Sri Aurobindo
or small openings on the surface and cystic hemorrhagic Institute of Medical Sciences, Indore, Madhya Pradesh, India, e-mail:
5
lesions in the cavity. In this case, an appearance exactly priyabhave1@gmail.com
similar to that described by Campo et al was observed on
hysteroscopy showing endometrial defects in the fundal area. Shilpa Sapre
While hysteroscopy alone cannot diagnose or rule out Associate Professor, Department of Obstetrics and Gynecology, Sri
adenomyosis, the typical endometrial lesions associated with Aurobindo Institute of Medical Sciences, Indore, Madhya Pradesh, India
it can aid in the diagnosis when accompanied by a
transvaginal ultrasound. This can enable clinicians to decide Shilpa Bhandari
on taking an endomyometrial biopsy when the hysteroscopic Associate Professor, Department of Reproductive Medicine, Sri
picture is suggestive of adenomyosis. Aurobindo Institute of Medical Sciences, Indore, Madhya Pradesh, India
104