
Page 20 - Journal of Laparoscopic Surgery - WALS Journal
P. 20
Nuhu Musa Mshelia et al
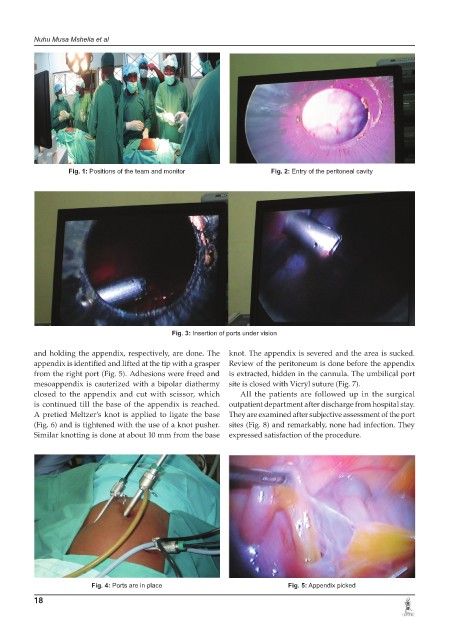
Fig. 1: Positions of the team and monitor Fig. 2: Entry of the peritoneal cavity
Fig. 3: Insertion of ports under vision
and holding the appendix, respectively, are done. The knot. The appendix is severed and the area is sucked.
appendix is identified and lifted at the tip with a grasper Review of the peritoneum is done before the appendix
from the right port (Fig. 5). Adhesions were freed and is extracted, hidden in the cannula. The umbilical port
mesoappendix is cauterized with a bipolar diathermy site is closed with Vicryl suture (Fig. 7).
closed to the appendix and cut with scissor, which All the patients are followed up in the surgical
is continued till the base of the appendix is reached. outpatient department after discharge from hospital stay.
A pretied Meltzer’s knot is applied to ligate the base They are examined after subjective assessment of the port
(Fig. 6) and is tightened with the use of a knot pusher. sites (Fig. 8) and remarkably, none had infection. They
Similar knotting is done at about 10 mm from the base expressed satisfaction of the procedure.
Fig. 4: Ports are in place Fig. 5: Appendix picked
18