
Page 12 - World Journal of Laparoscopic Surgery
P. 12
RK Mishra et al
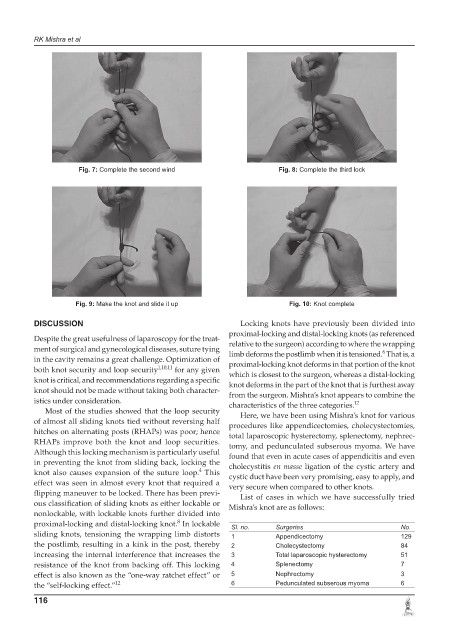
Fig. 7: Complete the second wind Fig. 8: Complete the third lock
Fig. 9: Make the knot and slide it up Fig. 10: Knot complete
DISCUSSION Locking knots have previously been divided into
proximallocking and distallocking knots (as referenced
Despite the great usefulness of laparoscopy for the treat relative to the surgeon) according to where the wrapping
ment of surgical and gynecological diseases, suture tying limb deforms the postlimb when it is tensioned. That is, a
6
in the cavity remains a great challenge. Optimization of proximallocking knot deforms in that portion of the knot
both knot security and loop security 1,10,11 for any given which is closest to the surgeon, whereas a distallocking
knot is critical, and recommendations regarding a specific knot deforms in the part of the knot that is furthest away
knot should not be made without taking both character from the surgeon. Mishra’s knot appears to combine the
istics under consideration. characteristics of the three categories. 12
Most of the studies showed that the loop security Here, we have been using Mishra’s knot for various
of almost all sliding knots tied without reversing half procedures like appendicectomies, cholecystectomies,
hitches on alternating posts (RHAPs) was poor; hence total laparoscopic hysterectomy, splenectomy, nephrec
RHAPs improve both the knot and loop securities. tomy, and pedunculated subserous myoma. We have
Although this locking mechanism is particularly useful found that even in acute cases of appendicitis and even
in preventing the knot from sliding back, locking the cholecystitis en masse ligation of the cystic artery and
4
knot also causes expansion of the suture loop. This cystic duct have been very promising, easy to apply, and
effect was seen in almost every knot that required a very secure when compared to other knots.
flipping maneuver to be locked. There has been previ List of cases in which we have successfully tried
ous classification of sliding knots as either lockable or Mishra’s knot are as follows:
nonlockable, with lockable knots further divided into
8
proximallocking and distallocking knot. In lockable Sl. no. Surgeries No.
sliding knots, tensioning the wrapping limb distorts 1 Appendicectomy 129
the postlimb, resulting in a kink in the post, thereby 2 Cholecystectomy 84
increasing the internal interference that increases the 3 Total laparoscopic hysterectomy 51
resistance of the knot from backing off. This locking 4 Splenectomy 7
effect is also known as the “oneway ratchet effect” or 5 Nephrectomy 3
the “selflocking effect.” 12 6 Pedunculated subserous myoma 6
116