
Page 43 - World Journal of Laparoscopic Surgery
P. 43
WJOLS
Laparoscopic Management of Stomach Sleeve Obstruction after Sleeve Gastrectomy
Fig. 2: Twisting (Clockwise) of sleeve at incisure angularis
intermittent stitches using 3–0 Vicryl. The gastropexy
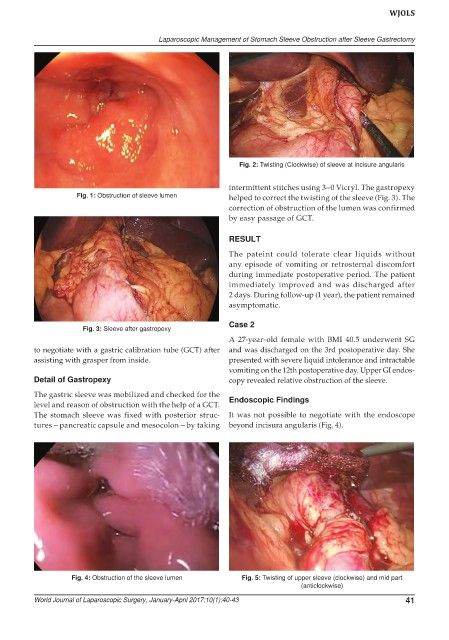
Fig. 1: Obstruction of sleeve lumen helped to correct the twisting of the sleeve (Fig. 3). The
correction of obstruction of the lumen was confirmed
by easy passage of GCT.
RESULT
The pateint could tolerate clear liquids without
any episode of vomiting or retrosternal discomfort
during immediate postoperative period. The patient
immediately improved and was discharged after
2 days. During follow-up (1 year), the patient remained
asymptomatic.
Case 2
Fig. 3: Sleeve after gastropexy
A 27-year-old female with BMI 40.5 underwent SG
to negotiate with a gastric calibration tube (GCT) after and was discharged on the 3rd postoperative day. She
assisting with grasper from inside. presented with severe liquid intolerance and intractable
vomiting on the 12th postoperative day. Upper GI endos-
Detail of Gastropexy copy revealed relative obstruction of the sleeve.
The gastric sleeve was mobilized and checked for the
level and reason of obstruction with the help of a GCT. Endoscopic Findings
The stomach sleeve was fixed with posterior struc- It was not possible to negotiate with the endoscope
tures – pancreatic capsule and mesocolon – by taking beyond incisura angularis (Fig. 4).
Fig. 4: Obstruction of the sleeve lumen Fig. 5: Twisting of upper sleeve (clockwise) and mid part
(anticlockwise)
World Journal of Laparoscopic Surgery, January-April 2017;10(1):40-43 41