
Page 44 - World Journal of Laparoscopic Surgery
P. 44
Sanjay Patolia, Ibrahim Hazza
Making the stomach free is a mandatory part of
the surgery; thus, it cannot be avoided, but crafting the
stomach sleeve with proper architecture can be focused
and undertaken to avoid obstruction.
Tips to create sleeve with proper shape:
• Drop the idea of performing SG when there is large
hiatus hernia and select gastric bypass.
• Do not overdissect posterior to antrum toward pylorus
because the free antrum can rotate anticlockwise very
easily resulting in obstruction at the level of incisura
angularis.
• The angle on the staple line between the 1st and 2nd
cartridge firing should be wide because a narrow
angle will not create a smooth distal passage.
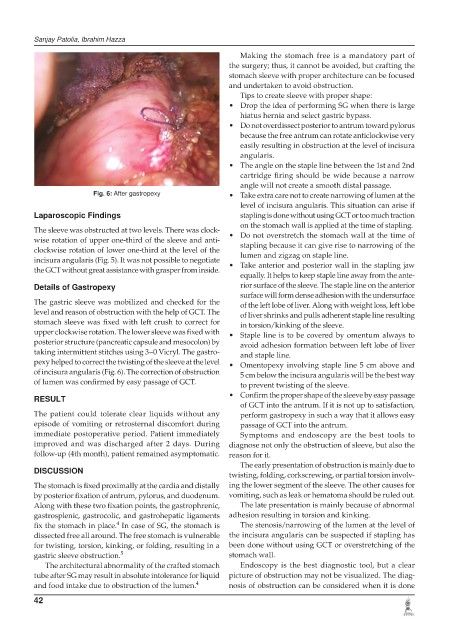
Fig. 6: After gastropexy • Take extra care not to create narrowing of lumen at the
level of incisura angularis. This situation can arise if
Laparoscopic Findings stapling is done without using GCT or too much traction
on the stomach wall is applied at the time of stapling.
The sleeve was obstructed at two levels. There was clock- • Do not overstretch the stomach wall at the time of
wise rotation of upper one-third of the sleeve and anti- stapling because it can give rise to narrowing of the
clockwise rotation of lower one-third at the level of the
incisura angularis (Fig. 5). It was not possible to negotiate lumen and zigzag on staple line.
the GCT without great assistance with grasper from inside. • Take anterior and posterior wall in the stapling jaw
equally. It helps to keep staple line away from the ante-
Details of Gastropexy rior surface of the sleeve. The staple line on the anterior
surface will form dense adhesion with the undersurface
The gastric sleeve was mobilized and checked for the of the left lobe of liver. Along with weight loss, left lobe
level and reason of obstruction with the help of GCT. The of liver shrinks and pulls adherent staple line resulting
stomach sleeve was fixed with left crush to correct for in torsion/kinking of the sleeve.
upper clockwise rotation. The lower sleeve was fixed with • Staple line is to be covered by omentum always to
posterior structure (pancreatic capsule and mesocolon) by avoid adhesion formation between left lobe of liver
taking intermittent stitches using 3–0 Vicryl. The gastro- and staple line.
pexy helped to correct the twisting of the sleeve at the level • Omentopexy involving staple line 5 cm above and
of incisura angularis (Fig. 6). The correction of obstruction 5 cm below the incisura angularis will be the best way
of lumen was confirmed by easy passage of GCT. to prevent twisting of the sleeve.
• Confirm the proper shape of the sleeve by easy passage
RESULT
of GCT into the antrum. If it is not up to satisfaction,
The patient could tolerate clear liquids without any perform gastropexy in such a way that it allows easy
episode of vomiting or retrosternal discomfort during passage of GCT into the antrum.
immediate postoperative period. Patient immediately Symptoms and endoscopy are the best tools to
improved and was discharged after 2 days. During diagnose not only the obstruction of sleeve, but also the
follow-up (4th month), patient remained asymptomatic. reason for it.
The early presentation of obstruction is mainly due to
DISCUSSION
twisting, folding, corkscrewing, or partial torsion involv-
The stomach is fixed proximally at the cardia and distally ing the lower segment of the sleeve. The other causes for
by posterior fixation of antrum, pylorus, and duodenum. vomiting, such as leak or hematoma should be ruled out.
Along with these two fixation points, the gastrophrenic, The late presentation is mainly because of abnormal
gastrosplenic, gastrocolic, and gastrohepatic ligaments adhesion resulting in torsion and kinking.
4
fix the stomach in place. In case of SG, the stomach is The stenosis/narrowing of the lumen at the level of
dissected free all around. The free stomach is vulnerable the incisura angularis can be suspected if stapling has
for twisting, torsion, kinking, or folding, resulting in a been done without using GCT or overstretching of the
gastric sleeve obstruction. 5 stomach wall.
The architectural abnormality of the crafted stomach Endoscopy is the best diagnostic tool, but a clear
tube after SG may result in absolute intolerance for liquid picture of obstruction may not be visualized. The diag-
and food intake due to obstruction of the lumen. 4 nosis of obstruction can be considered when it is done
42