Laparoscopic Scissors
Jean-Claude Margueron of Emar in the 14th century BC invented scissors. Scissors are one of the oldest surgical instruments used by surgeons. Scissors are used to perform many tasks in open surgical procedure but its use in minimal access surgery is restricted. In minimal access surgery, scissors require greater skill because in inexperienced hands it may cause unnecessary bleeding and damage to important structures.
Mechanism of Cutting
The scissors has three parts:
1. Blade
2. Fulcrum
3. Handle.
The cutting force of the scissors works on the law of the lever. The force applied on the blade can be calculated by the length of the handle and force applied on the grip of the handle. A pair of scissors is an example of first-class levers connected together at the joint known as the fulcrum.
There are three types of lever.
Scissors works on the principle of class 1 lever. In class 1 lever, the Pivot (fulcrum) is between the effort and the load. The more length of the handle or the fulcrum of the scissors, the less force of cutting will be required. The laparoscopic scissors do not apply the exact law of lever because of the cylinder action of the long shaft, but the design of the handle helps in the amplification of force by lever action.
Scissors function by the combination of:
• Gripping
• Squeezing
• Tearing.
When the blades of scissors close, its sharp edges grind against each other and any tissue which comes between the blades of scissors will get cut. Scissors-tissue interaction can be described in five stages:
Engagement
In the process of engagement, the two blades of the scissors engage a piece of tissue to cut. The amount of tissue engaged should not be more than the space between the jaw of blades otherwise the chance of slipping of tissue is more. After the engagement, the force applied on the handle of the scissors initiates cutting.
Elastic Deformation
This stage starts just after the engagement of tissue between the blades of the scissors. In this process, the tissues between the two blades of scissors start deforming. This stage is called elastic deformation, because if the force on the handle of scissors is removed then the tissue deformity will return to its normal state.
Plastic Deformation
Further force on the handle of scissors will cause the tissue between the blades to go into a plastically deformed state, which is irreversible. After undergoing this state of tissue deformation, even if the further process of cutting is stopped the impression on the tissue remains.
Fracture
Further increased force on the fulcrum of scissors will result in the fracture of the intercellular plane of the tissue. This stage of cutting is peculiar to scissors because unlike the scalpel, the site of tissue fracture is intercellular.
Separation
After the fracture, the tissue separates along the line of the blade of scissors, and then this whole process of cutting will continue on the engaged tissue.
Histology of the Tissue After Cutting
Histological examination of the tissue after cutting with scissors shows that there is the separation of tissue through the intracellular plane. Microscopic examination shows a serrated cut margin along the line of tissue separation.
Types of Laparoscopic Scissors:
Straight Scissor
The blade of this scissor is straight and it is widely used as an instrument for mechanical dissection in laparoscopic surgery.
Straight scissor can give a controlled depth of cutting because it has only one moving jaw. At the time of cutting the fixed jaw should be down and moving jaw should be up.

Straight Scissor
Curved Scissor
The blade of these scissors is slightly curved and this is the most widely used scissor in laparoscopic surgery.
Curved Scissor
These scissors are mounted on a curved handle which is either fixed or retractable. The type with a fixed curvature proximal to the scissor blades requires an introduction through flexible valveless ports. The surgeon prefers this scissor because the curvature of the blade of the scissors abolishes the angle of laparoscopic instrument manipulation and a better view through the telescope is achieved.
Serrated Scissor
The main advantage of these scissors is that the serrated edges prevent the tissue to slip out of the blades. It is a useful instrument in cutting a slippery tissue or ligature. Serrated scissors may be straight or curved.

Serrated Scissor
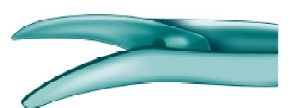
Hook Scissor
The sharp edge of both blades is in the shape of a flattened C. The blades can be partially closed, trapping tissue in the hollow of the blades without dividing it and allowing it to be slightly retracted. This allows the surgeon to double-check before he closes the blades completely. The main advantage of this scissors is that it encircles the structure before cutting: Tissue is held between its jaws and there is no chance of slipping. The hook scissor is especially useful for cutting a secured duct or artery in laparoscopic surgery. The cutting of the nerve bundles in neurectomy becomes very easy with the help of this scissor. Hook scissors are also helpful in the partial cutting of cystic duct for intraoperative cholangiography. All the other scissors cut from proximal to distal whereas the hook scissors cut distal to proximal.
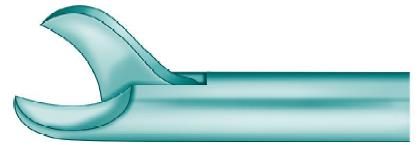
Hook Scissor
Micro-Tip Scissor
These very fine scissors, are either straight or angled, and are used to partially transect the cystic duct. The main advantage of this scissor is to cut the ducts partially for facilitating cannulation. It may be used for cutting the cystic duct for performing intraoperative cholangiogram. Exploration of small ducts like a common bile duct is very helpful with microscissors due to its fine small blades. Fine microscissors are also available in their curved form.

Microtip Scissor
The use of scissors endoscopically requires little modification of open techniques.
The basic instrument is a miniaturized, long-handled version of conventional scissors and can be single or double action. There are some special types of scissors used in endoscopic surgery.
Insulated Scissors
These allow the use of electrocautery through the scissors. However, when using non-disposable instruments, electrocoagulation using the open blades leads to the blunting of the edges. Electrocoagulation using the scissors is thus limited, and when carried out is applied only with the blades closed. Scissor dissection is usually carried out with a grasper on the other hand. If this instrument is insulated then any vessels encountered can be easily coagulated by the grasper. A further disadvantage associated with electrocoagulation with the scissors results from the long non-insulated segment required to accommodate the blades and hinge mechanism. For safe practice, this requires to be kept in view, and this limits the magnification available to the surgeon.
Scissors have following advantages:
• Inexpensive
• Safe in safe hand
• Operator determined precise action
• Closed blades can work for blunt dissection and electrocautery
• Piercing tissue with closed blades and then opening helps in obtaining a good plane of dissection.
Scissors have following disadvantages:
• Non-hemostatic
• Accidental chances of cutting small ducts and vessels
• If overlooked, due to its pointed end, there is a chance of injury to viscera
• If used for electric coagulation, its blades get blunt easily.
Jean-Claude Margueron of Emar in the 14th century BC invented scissors. Scissors are one of the oldest surgical instruments used by surgeons. Scissors are used to perform many tasks in open surgical procedure but its use in minimal access surgery is restricted. In minimal access surgery, scissors require greater skill because in inexperienced hands it may cause unnecessary bleeding and damage to important structures.
Mechanism of Cutting
The scissors has three parts:
1. Blade
2. Fulcrum
3. Handle.
The cutting force of the scissors works on the law of the lever. The force applied on the blade can be calculated by the length of the handle and force applied on the grip of the handle. A pair of scissors is an example of first-class levers connected together at the joint known as the fulcrum.
There are three types of lever.
Scissors works on the principle of class 1 lever. In class 1 lever, the Pivot (fulcrum) is between the effort and the load. The more length of the handle or the fulcrum of the scissors, the less force of cutting will be required. The laparoscopic scissors do not apply the exact law of lever because of the cylinder action of the long shaft, but the design of the handle helps in the amplification of force by lever action.
Scissors function by the combination of:
• Gripping
• Squeezing
• Tearing.
When the blades of scissors close, its sharp edges grind against each other and any tissue which comes between the blades of scissors will get cut. Scissors-tissue interaction can be described in five stages:
Engagement
In the process of engagement, the two blades of the scissors engage a piece of tissue to cut. The amount of tissue engaged should not be more than the space between the jaw of blades otherwise the chance of slipping of tissue is more. After the engagement, the force applied on the handle of the scissors initiates cutting.
Elastic Deformation
This stage starts just after the engagement of tissue between the blades of the scissors. In this process, the tissues between the two blades of scissors start deforming. This stage is called elastic deformation, because if the force on the handle of scissors is removed then the tissue deformity will return to its normal state.
Plastic Deformation
Further force on the handle of scissors will cause the tissue between the blades to go into a plastically deformed state, which is irreversible. After undergoing this state of tissue deformation, even if the further process of cutting is stopped the impression on the tissue remains.
Fracture
Further increased force on the fulcrum of scissors will result in the fracture of the intercellular plane of the tissue. This stage of cutting is peculiar to scissors because unlike the scalpel, the site of tissue fracture is intercellular.
Separation
After the fracture, the tissue separates along the line of the blade of scissors, and then this whole process of cutting will continue on the engaged tissue.
Histology of the Tissue After Cutting
Histological examination of the tissue after cutting with scissors shows that there is the separation of tissue through the intracellular plane. Microscopic examination shows a serrated cut margin along the line of tissue separation.
Types of Laparoscopic Scissors:
Straight Scissor
The blade of this scissor is straight and it is widely used as an instrument for mechanical dissection in laparoscopic surgery.
Straight scissor can give a controlled depth of cutting because it has only one moving jaw. At the time of cutting the fixed jaw should be down and moving jaw should be up.
Straight Scissor
Curved Scissor
The blade of these scissors is slightly curved and this is the most widely used scissor in laparoscopic surgery.
Curved Scissor
These scissors are mounted on a curved handle which is either fixed or retractable. The type with a fixed curvature proximal to the scissor blades requires an introduction through flexible valveless ports. The surgeon prefers this scissor because the curvature of the blade of the scissors abolishes the angle of laparoscopic instrument manipulation and a better view through the telescope is achieved.
Serrated Scissor
The main advantage of these scissors is that the serrated edges prevent the tissue to slip out of the blades. It is a useful instrument in cutting a slippery tissue or ligature. Serrated scissors may be straight or curved.
Serrated Scissor
Hook Scissor
The sharp edge of both blades is in the shape of a flattened C. The blades can be partially closed, trapping tissue in the hollow of the blades without dividing it and allowing it to be slightly retracted. This allows the surgeon to double-check before he closes the blades completely. The main advantage of this scissors is that it encircles the structure before cutting: Tissue is held between its jaws and there is no chance of slipping. The hook scissor is especially useful for cutting a secured duct or artery in laparoscopic surgery. The cutting of the nerve bundles in neurectomy becomes very easy with the help of this scissor. Hook scissors are also helpful in the partial cutting of cystic duct for intraoperative cholangiography. All the other scissors cut from proximal to distal whereas the hook scissors cut distal to proximal.
Hook Scissor
Micro-Tip Scissor
These very fine scissors, are either straight or angled, and are used to partially transect the cystic duct. The main advantage of this scissor is to cut the ducts partially for facilitating cannulation. It may be used for cutting the cystic duct for performing intraoperative cholangiogram. Exploration of small ducts like a common bile duct is very helpful with microscissors due to its fine small blades. Fine microscissors are also available in their curved form.
Microtip Scissor
The use of scissors endoscopically requires little modification of open techniques.
The basic instrument is a miniaturized, long-handled version of conventional scissors and can be single or double action. There are some special types of scissors used in endoscopic surgery.
Insulated Scissors
These allow the use of electrocautery through the scissors. However, when using non-disposable instruments, electrocoagulation using the open blades leads to the blunting of the edges. Electrocoagulation using the scissors is thus limited, and when carried out is applied only with the blades closed. Scissor dissection is usually carried out with a grasper on the other hand. If this instrument is insulated then any vessels encountered can be easily coagulated by the grasper. A further disadvantage associated with electrocoagulation with the scissors results from the long non-insulated segment required to accommodate the blades and hinge mechanism. For safe practice, this requires to be kept in view, and this limits the magnification available to the surgeon.
Scissors have following advantages:
• Inexpensive
• Safe in safe hand
• Operator determined precise action
• Closed blades can work for blunt dissection and electrocautery
• Piercing tissue with closed blades and then opening helps in obtaining a good plane of dissection.
Scissors have following disadvantages:
• Non-hemostatic
• Accidental chances of cutting small ducts and vessels
• If overlooked, due to its pointed end, there is a chance of injury to viscera
• If used for electric coagulation, its blades get blunt easily.

