Hand-assisted Laparoscopic Surgery
Introduction
In hand-assisted surgery, the surgeon can insert a hand through a small incision via a special pressurized sleeve. The surgeon makes a small incision in the abdomen and inserts his hand into the patient’s body. Hand-assisted laparoscopic surgery (HALS) devices allow for the introduction of the surgeon’s non-dominant hand into the peritoneal cavity without loss of the pneumoperitoneum. The use of hand-assisted techniques in difficult cases facilitates the surgical procedure and offers an interesting alternative to the purely laparoscopic approach.
Hand-assisted laparoscopic surgery allows for a reduction in the number of trocars compared to the purely laparoscopic approach. The proper placement of the hand- assist device is one of the fundamental principles of HALS. The hand-assisted device should never be placed directly over the operative field. According to the principle of triangulation, the hand-assisted device is ideally placed in the same position as that of the nondominant operating trocar in the purely laparoscopic approach.
The hand is ideal for sensory perception and to guide the surgical instruments. The surgeon can manipulate with his other hand while observing the procedure on a monitor. With both a hand and laparoscopic instruments doing the work, the surgeon has more control over the operation and sense of depth and sensation of touch which cannot be gained through the lens of a camera. The large organ can be removed intact, making it possible to evaluate cancer. The hand-assisted approach is also considered better for surgeons who are still learning laparoscopic techniques. Hand-assisted laparoscopic surgery is the use of the nondominant hand intra-abdominally, together with the laparoscopic instruments in the dominant hand.
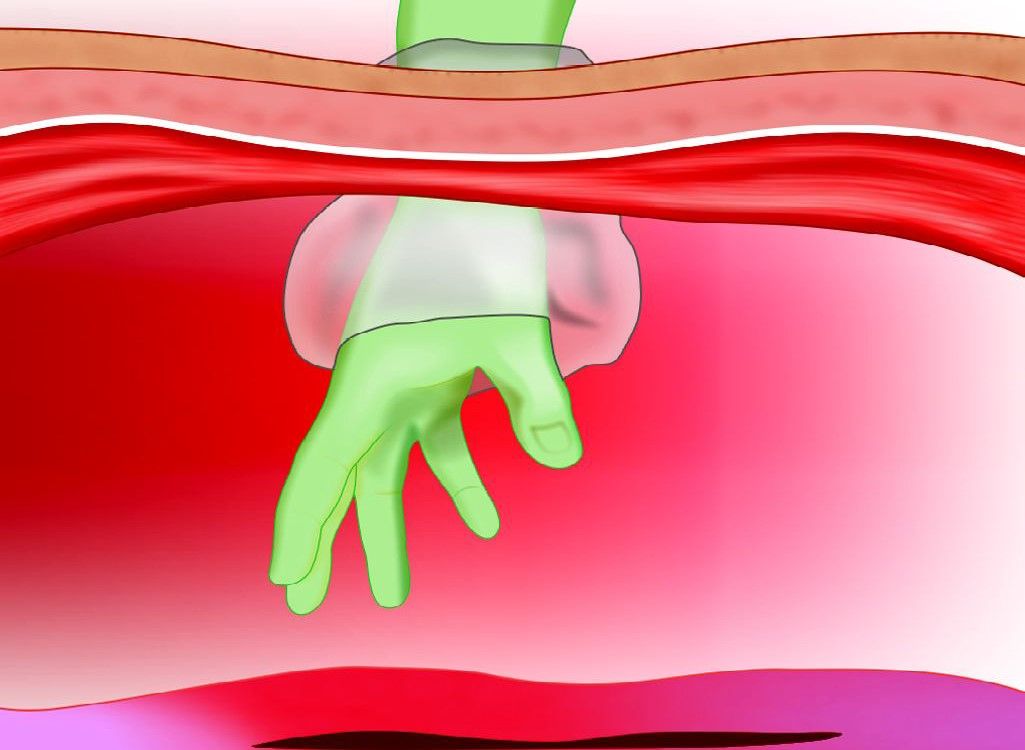
Positioning through the abdominal wall

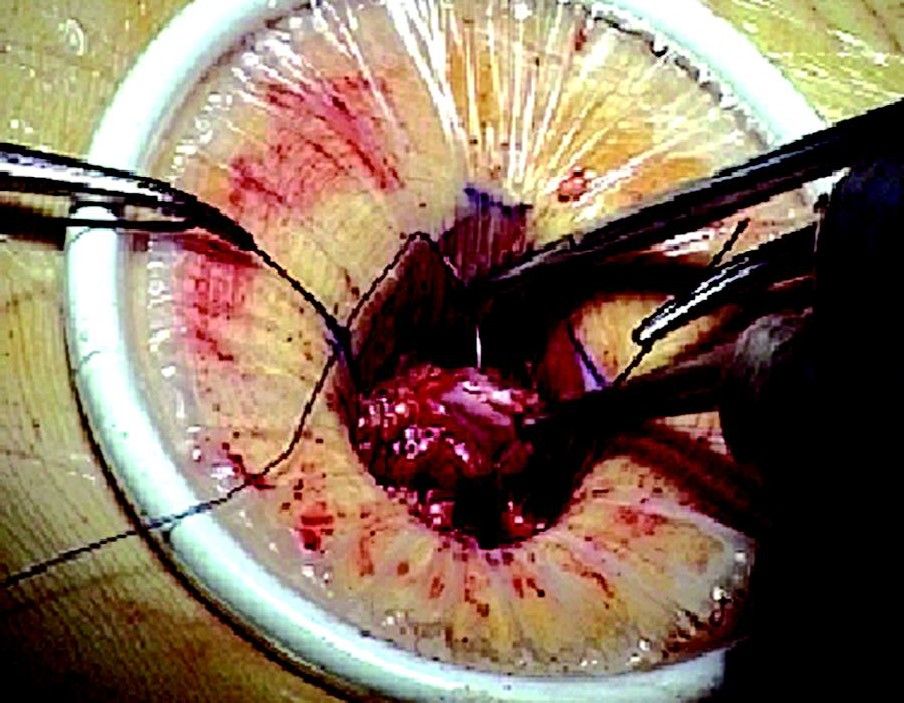
Introduction of instruments
Working through the port
The introduction of the surgeon’s hand via the hand-assisted device allows for tactile feedback and complements the information obtained visually. Hand-assisted laparoscopic surgery greatly facilitates the mobilization of the organs and helps for the identification of proper dissection plane, thus minimizing oozing and blood loss. Hand-assisted laparoscopic surgery offers several real advantages during the procedure resulting in a significant time gain. This is especially true in obese patients as well as in cases of significant abdominal adhesions.
The size of the incision for placement of the hand cannula is determined by the size of the surgeon’s glove. A retractor- protractor which is an open-ended plastic cylinder with a malleable ring at each end is then introduced into the abdominal cavity through the incision. This provides a seal for the skin wound both at the peritoneal and skin sites and keeps the incision open and also protects the wound against contamination by bacteria and malignant cells. The pneumosleeve is fitted underhand cannula and manipulated to achieve the best possible angle for the surgeon’s arm during dissection. The adhesive packing is removed and the flanges are secured to the skin. A one-way valve located in the sleeve’s lumen prevents gas from escaping from the abdomen.
An additional cover is placed on the surgeon’s arm, which is impermeable to gas. The pneumosleeve is entered and secured to the surgeon’s upper arm by means of a Velcro band to prevent gas escape. The hand is then placed through the hand cannula into the abdomen. Hand-assisted laparoscopic surgery (HALS), open and laparoscopic procedure is compared in the table below.
Hand-assisted laparoscopic surgery (HALS) is the use of the non-dominant hand through a hand port device. It is an important adjunctive tool with other laparoscopic instruments. The hand port will be fixed via a mini-laparotomy incision, aiming for safe maintenance of intra-abdominal gas throughout the operative procedure. The main indication for HALS is in advanced and complex laparoscopic surgical procedures. The rationale behind HALS is that laparoscopic surgery can be used for both simple and complex procedures.
Disadvantages of total laparoscopic surgery:
• Loss of direct tactile sensation
• Difficult hand-eye coordination
• Multiple times instrument change
• Conversion rate in complex abdominal procedures.
“Hand port” system allows surgeons the ability to insert a hand into the patient to gain a tactile sense during laparoscopic surgical procedures. This is a real improvement over previous techniques which precluded a surgeon from gaining information through touch. Commercially available to date and approved by the FDA are Dexterity Device, Intromit, Hand port, and Omni port. Omni port has been extensively studied by Europe University, Dundee University as well as being clinically applied with success in the repair of abdominal aortic aneurysms in Germany and the USA. The pneumo-access bubble is one of the great advances by Cuschieri and Shapiro, allowing complete visual access with the hand inside and pneumoperitoneum safely maintained.
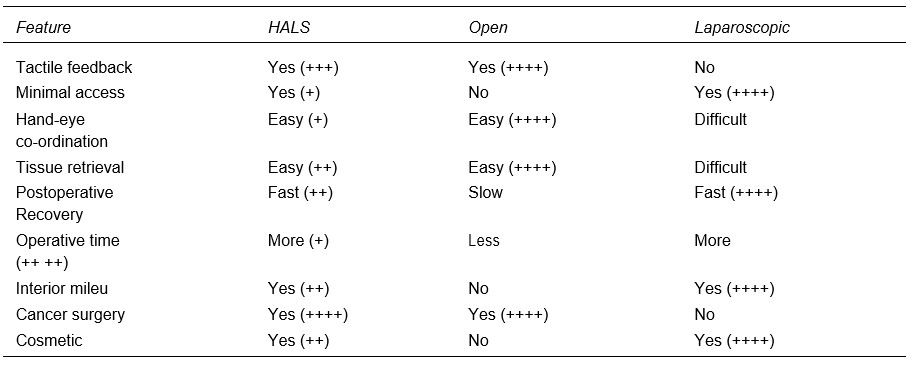
Comparison of HALS, open and laparoscopic procedure
Hand Port Devices
Devices connected to abdomen by adhesive flange:
• Dexterity (Inc., Roswell, GA, USA)
• IntroMit (Medtech Ltd., Dublin, Ireland).
Kissing Balloon Principle
Hand port device (Smith-Nephew PLC, England).
Single Piece Devices
• LapDisc (Hakko Medical, Japan)
• Omni port (Advanced Surgical Concepts Ltd., Ireland).
The IntroMit is a single-piece device that requires an adhesive to be secured to the body wall. There is no sleeve required and the device can be placed without a pneumoperitoneum.
In the Hand port system, the surgeon must wear a sleeve that attaches to the inflatable base of the device. Insertion or removal of the hand from the abdomen requires removal of the sleeve from the device, causing an immediate loss of pneumoperitoneum.
The Gel port is a three-piece device that uses a wound protecting sheath (inner ring), a wound retractor (outer ring), and a gel seal cap that affixes to the wound retractor. The seal that is created maintains pneumoperitoneum, even without the insertion of the surgeon’s hand. Removal of the surgeon’s hand from the abdominal cavity does not cause loss of pneumoperitoneum. Moreover, the gel seal cap can be pierced by a trocar or accessory instrument while maintaining a seal at the puncture site. The large surface area of this device requires an adequate area for application on the body wall and may not be ideal for lower-quadrant hand incisions in smaller patients. However, a unique benefit of this device is that it permits the insertion instruments through the gel seal cap even while the hand is inserted in the abdomen.
The Omni port is an inflatable device through which the surgeon can rapidly remove and reinsert the hand without losing pneumoperitoneum. The device also can be insufflated to maintain pneumoperitoneum without hand insertion, allowing an accessory trocar and instrument to be inserted through this device. The LapDisc consists of inner and middle rings that are connected by a silicone membrane spanning the abdominal wall. A third outermost ring rotates on the middle ring and acts as an iris, which is tightened to seal the device around the surgeon’s arm. There are no pieces that require assembly with this device and insertion is quick and simple. This device has the smallest diameter (12 cm) and can be placed on most abdominal walls without interfering with the placement of adjacent trocars.
Hand-Assisted Laparoscopic Surgery

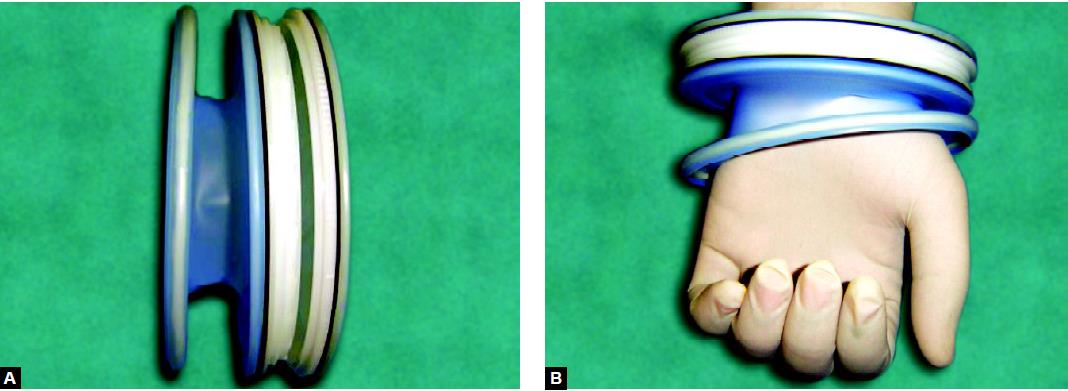
Omni port inflated

Omni port deflated
Omni Port
Omni port is the preferred device because it is:
• Single
• Simple component
• Easy to insert
• Comfortable
• Efficient pneumatic seal.
Indication of HALS
Hand-assisted laparoscopic surgery is a new addition to minimal access surgery. It has great potential. Many surgical operations, from the simplest to the very complicated, are greatly facilitated by the introduction of the hand into the laparoscopic arena. It is therefore purposefully designed in assisting the surgeon for a complex intra-abdominal operation to be done with total laparoscopy. It stimulated many vascular surgeons throughout the world to reintroduce it into the repair of complex and challenging abdominal vasculature. Nephrectomy, splenectomy, colorectal surgeries are nicely performed through the hand-assisted technique.

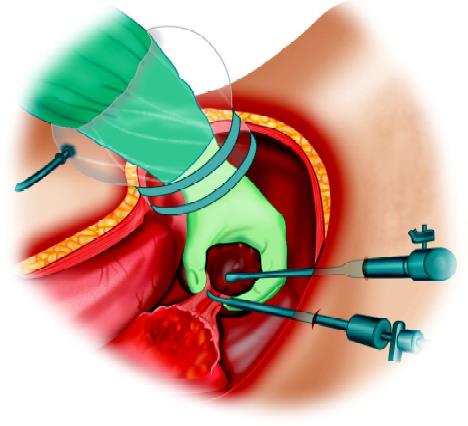
HALS with Omni port
Advantage of HALS
• Restored tactile feedback
• Preserving the main idea of minimal access surgery (MAS)
• A mini-laparotomy hand port incision
• Reduced conversion rate in total laparoscopy
• Enhanced safety and efficiency allowing the completion of the operation with a hand inside
• Maintenance of the intra-abdominal pressure to facilitate the better view and magnification of a laparoscopic telescope
• Improving the steep learning curve for inexperienced surgeons
• Promising reduced cost-benefit ratio.
Limitations of HALS
Limitations can be summarized as:
• Fatigue
• Possible impaired tactile feedback through a long complex procedure
• Minor ergonomic restriction is due to the crowdedness of the hand with the instruments
• Not well accepted by patients and surgeons because there is already a mini-laparotomy.
• Cosmetically inferior to total laparoscopic surgery.
Lapdisc Hand Access Device
This essential product information sheet does not include all of the information necessary for the selection and use of a device.
LapDisc
Indications
• The LapDisc hand access device is intended to provide an extracorporeal extension of pneumoperitoneum and abdominal access for the surgeon during laparoscopic surgery.
• The LapDisc is indicated for use in laparoscopic procedures, where entry of the surgeon’s hand may facilitate the procedure, and for extraction of large specimens.
• The LapDisc has an application in colorectal, urological, and general surgical procedures. This indication for use includes the specific procedures which fall under these broad categories.
Contraindications: None knew.
Warnings and Precautions
• Minimally invasive procedures should be performed only by persons having adequate training and familiarity with minimally invasive techniques, including laparoscopic, hand-assisted laparoscopic, and open surgical procedures. Consult medical literature relative to techniques, complications, and hazards prior to the performance of any minimally invasive procedure.
• Minimally invasive instruments may vary from manufacturer to manufacturer. When minimally invasive instruments and accessories from different manufacturers are employed together in a procedure, verify compatibility prior to initiation of the procedure.
• A thorough understanding of the principles and techniques involved in laser, electrosurgical, and ultrasonic procedures is essential to avoid shock and burn hazards to both patient and medical personnel and damage to the device or other medical instruments. Ensure that electrical insulation or grounding is not compromised. Do not immerse electrosurgical instruments in liquid unless they are designed and labeled to be immersed.
LD111-Precaution
• This device should not be used in patients with abdominal wall thickness greater than 5 cm, or incisions less than 5 cm in length.
• Do not use the device where the incision length is greater than 9 cm as loss of pneumoperitoneum may occur.
LD112-Precaution
• This device should be used in patients with abdominal wall thickness greater than 5 cm and less than or equal to 9 cm.
• Do not use the device where the incision length is greater than 9 cm as loss of pneumoperitoneum may occur.
• If pneumoperitoneum occurs:
1. Fully close the iris valve
2. Place damp gauze underneath the LapDisc, between the lower ring and the fascia, to stop the airflow.
• Do not allow sharp instruments such as forceps to come in contact with the silicone rubber sleeves as puncture or tearing may occur.
• Do not lay surgical instruments on the LapDisc or allow metal or sharp surgical instruments to come in contact with the LapDisc as this may weaken or damage the flexible silicone membranes.
• Sterile, water-soluble lubricant should be applied to the dorsum of the gloved hand prior to insertion through the LapDisc. Unlubricated hands may cause significant friction and tear the device.
• Do not remove the hand with the iris valve closed as it may tear the device.
• Do not overtighten the iris valve.
• Use caution when opening the iris valve when the abdomen is insufflated, as rapid loss of pneumoperitoneum may occur.
• After removing the instrument, inspect the site for hemostasis. If hemostasis is not present, appropriate techniques should be used to achieve hemostasis.
• Instruments or devices which come into contact with bodily fluids may require special disposal handling to prevent biological contamination.
• Dispose of all opened instruments whether used or unused. Do not resterilize the instrument. Resterilization may compromise the integrity of the device which may result in unintended injury.
Future Prospect of HALS
There are general and specific limitations, awaiting multicenter prospective randomized trials in order to compare HALS in various major intra-abdominal procedures with the traditional open surgery. Hand-assisted laparoscopic surgery (HALS) can be used for all major complex abdominal surgeries like:
• Splenectomy
• Nephrectomy
• Morbid obesity surgery
• Pancreatectomy
• Nissen fundoplication
• Esophagectomy
• Rectopexy
• Repair of abdominal aortic aneurysm.
Hand-assisted laparoscopic surgery is technically much easier than total laparoscopy in advanced abdominal procedures. It can help the beginning laparoscopic surgeon to practice such major operations.

Hemicolectomy with HALS
Introduction
In hand-assisted surgery, the surgeon can insert a hand through a small incision via a special pressurized sleeve. The surgeon makes a small incision in the abdomen and inserts his hand into the patient’s body. Hand-assisted laparoscopic surgery (HALS) devices allow for the introduction of the surgeon’s non-dominant hand into the peritoneal cavity without loss of the pneumoperitoneum. The use of hand-assisted techniques in difficult cases facilitates the surgical procedure and offers an interesting alternative to the purely laparoscopic approach.
Hand-assisted laparoscopic surgery allows for a reduction in the number of trocars compared to the purely laparoscopic approach. The proper placement of the hand- assist device is one of the fundamental principles of HALS. The hand-assisted device should never be placed directly over the operative field. According to the principle of triangulation, the hand-assisted device is ideally placed in the same position as that of the nondominant operating trocar in the purely laparoscopic approach.
The hand is ideal for sensory perception and to guide the surgical instruments. The surgeon can manipulate with his other hand while observing the procedure on a monitor. With both a hand and laparoscopic instruments doing the work, the surgeon has more control over the operation and sense of depth and sensation of touch which cannot be gained through the lens of a camera. The large organ can be removed intact, making it possible to evaluate cancer. The hand-assisted approach is also considered better for surgeons who are still learning laparoscopic techniques. Hand-assisted laparoscopic surgery is the use of the nondominant hand intra-abdominally, together with the laparoscopic instruments in the dominant hand.
Positioning through the abdominal wall
Introduction of instruments
Working through the port
The introduction of the surgeon’s hand via the hand-assisted device allows for tactile feedback and complements the information obtained visually. Hand-assisted laparoscopic surgery greatly facilitates the mobilization of the organs and helps for the identification of proper dissection plane, thus minimizing oozing and blood loss. Hand-assisted laparoscopic surgery offers several real advantages during the procedure resulting in a significant time gain. This is especially true in obese patients as well as in cases of significant abdominal adhesions.
The size of the incision for placement of the hand cannula is determined by the size of the surgeon’s glove. A retractor- protractor which is an open-ended plastic cylinder with a malleable ring at each end is then introduced into the abdominal cavity through the incision. This provides a seal for the skin wound both at the peritoneal and skin sites and keeps the incision open and also protects the wound against contamination by bacteria and malignant cells. The pneumosleeve is fitted underhand cannula and manipulated to achieve the best possible angle for the surgeon’s arm during dissection. The adhesive packing is removed and the flanges are secured to the skin. A one-way valve located in the sleeve’s lumen prevents gas from escaping from the abdomen.
An additional cover is placed on the surgeon’s arm, which is impermeable to gas. The pneumosleeve is entered and secured to the surgeon’s upper arm by means of a Velcro band to prevent gas escape. The hand is then placed through the hand cannula into the abdomen. Hand-assisted laparoscopic surgery (HALS), open and laparoscopic procedure is compared in the table below.
Hand-assisted laparoscopic surgery (HALS) is the use of the non-dominant hand through a hand port device. It is an important adjunctive tool with other laparoscopic instruments. The hand port will be fixed via a mini-laparotomy incision, aiming for safe maintenance of intra-abdominal gas throughout the operative procedure. The main indication for HALS is in advanced and complex laparoscopic surgical procedures. The rationale behind HALS is that laparoscopic surgery can be used for both simple and complex procedures.
Disadvantages of total laparoscopic surgery:
• Loss of direct tactile sensation
• Difficult hand-eye coordination
• Multiple times instrument change
• Conversion rate in complex abdominal procedures.
“Hand port” system allows surgeons the ability to insert a hand into the patient to gain a tactile sense during laparoscopic surgical procedures. This is a real improvement over previous techniques which precluded a surgeon from gaining information through touch. Commercially available to date and approved by the FDA are Dexterity Device, Intromit, Hand port, and Omni port. Omni port has been extensively studied by Europe University, Dundee University as well as being clinically applied with success in the repair of abdominal aortic aneurysms in Germany and the USA. The pneumo-access bubble is one of the great advances by Cuschieri and Shapiro, allowing complete visual access with the hand inside and pneumoperitoneum safely maintained.
Comparison of HALS, open and laparoscopic procedure
Hand Port Devices
Devices connected to abdomen by adhesive flange:
• Dexterity (Inc., Roswell, GA, USA)
• IntroMit (Medtech Ltd., Dublin, Ireland).
Kissing Balloon Principle
Hand port device (Smith-Nephew PLC, England).
Single Piece Devices
• LapDisc (Hakko Medical, Japan)
• Omni port (Advanced Surgical Concepts Ltd., Ireland).
The IntroMit is a single-piece device that requires an adhesive to be secured to the body wall. There is no sleeve required and the device can be placed without a pneumoperitoneum.
In the Hand port system, the surgeon must wear a sleeve that attaches to the inflatable base of the device. Insertion or removal of the hand from the abdomen requires removal of the sleeve from the device, causing an immediate loss of pneumoperitoneum.
The Gel port is a three-piece device that uses a wound protecting sheath (inner ring), a wound retractor (outer ring), and a gel seal cap that affixes to the wound retractor. The seal that is created maintains pneumoperitoneum, even without the insertion of the surgeon’s hand. Removal of the surgeon’s hand from the abdominal cavity does not cause loss of pneumoperitoneum. Moreover, the gel seal cap can be pierced by a trocar or accessory instrument while maintaining a seal at the puncture site. The large surface area of this device requires an adequate area for application on the body wall and may not be ideal for lower-quadrant hand incisions in smaller patients. However, a unique benefit of this device is that it permits the insertion instruments through the gel seal cap even while the hand is inserted in the abdomen.
The Omni port is an inflatable device through which the surgeon can rapidly remove and reinsert the hand without losing pneumoperitoneum. The device also can be insufflated to maintain pneumoperitoneum without hand insertion, allowing an accessory trocar and instrument to be inserted through this device. The LapDisc consists of inner and middle rings that are connected by a silicone membrane spanning the abdominal wall. A third outermost ring rotates on the middle ring and acts as an iris, which is tightened to seal the device around the surgeon’s arm. There are no pieces that require assembly with this device and insertion is quick and simple. This device has the smallest diameter (12 cm) and can be placed on most abdominal walls without interfering with the placement of adjacent trocars.
Hand-Assisted Laparoscopic Surgery
Omni port inflated
Omni port deflated
Omni Port
Omni port is the preferred device because it is:
• Single
• Simple component
• Easy to insert
• Comfortable
• Efficient pneumatic seal.
Indication of HALS
Hand-assisted laparoscopic surgery is a new addition to minimal access surgery. It has great potential. Many surgical operations, from the simplest to the very complicated, are greatly facilitated by the introduction of the hand into the laparoscopic arena. It is therefore purposefully designed in assisting the surgeon for a complex intra-abdominal operation to be done with total laparoscopy. It stimulated many vascular surgeons throughout the world to reintroduce it into the repair of complex and challenging abdominal vasculature. Nephrectomy, splenectomy, colorectal surgeries are nicely performed through the hand-assisted technique.
HALS with Omni port
Advantage of HALS
• Restored tactile feedback
• Preserving the main idea of minimal access surgery (MAS)
• A mini-laparotomy hand port incision
• Reduced conversion rate in total laparoscopy
• Enhanced safety and efficiency allowing the completion of the operation with a hand inside
• Maintenance of the intra-abdominal pressure to facilitate the better view and magnification of a laparoscopic telescope
• Improving the steep learning curve for inexperienced surgeons
• Promising reduced cost-benefit ratio.
Limitations of HALS
Limitations can be summarized as:
• Fatigue
• Possible impaired tactile feedback through a long complex procedure
• Minor ergonomic restriction is due to the crowdedness of the hand with the instruments
• Not well accepted by patients and surgeons because there is already a mini-laparotomy.
• Cosmetically inferior to total laparoscopic surgery.
Lapdisc Hand Access Device
This essential product information sheet does not include all of the information necessary for the selection and use of a device.
LapDisc
Indications
• The LapDisc hand access device is intended to provide an extracorporeal extension of pneumoperitoneum and abdominal access for the surgeon during laparoscopic surgery.
• The LapDisc is indicated for use in laparoscopic procedures, where entry of the surgeon’s hand may facilitate the procedure, and for extraction of large specimens.
• The LapDisc has an application in colorectal, urological, and general surgical procedures. This indication for use includes the specific procedures which fall under these broad categories.
Contraindications: None knew.
Warnings and Precautions
• Minimally invasive procedures should be performed only by persons having adequate training and familiarity with minimally invasive techniques, including laparoscopic, hand-assisted laparoscopic, and open surgical procedures. Consult medical literature relative to techniques, complications, and hazards prior to the performance of any minimally invasive procedure.
• Minimally invasive instruments may vary from manufacturer to manufacturer. When minimally invasive instruments and accessories from different manufacturers are employed together in a procedure, verify compatibility prior to initiation of the procedure.
• A thorough understanding of the principles and techniques involved in laser, electrosurgical, and ultrasonic procedures is essential to avoid shock and burn hazards to both patient and medical personnel and damage to the device or other medical instruments. Ensure that electrical insulation or grounding is not compromised. Do not immerse electrosurgical instruments in liquid unless they are designed and labeled to be immersed.
LD111-Precaution
• This device should not be used in patients with abdominal wall thickness greater than 5 cm, or incisions less than 5 cm in length.
• Do not use the device where the incision length is greater than 9 cm as loss of pneumoperitoneum may occur.
LD112-Precaution
• This device should be used in patients with abdominal wall thickness greater than 5 cm and less than or equal to 9 cm.
• Do not use the device where the incision length is greater than 9 cm as loss of pneumoperitoneum may occur.
• If pneumoperitoneum occurs:
1. Fully close the iris valve
2. Place damp gauze underneath the LapDisc, between the lower ring and the fascia, to stop the airflow.
• Do not allow sharp instruments such as forceps to come in contact with the silicone rubber sleeves as puncture or tearing may occur.
• Do not lay surgical instruments on the LapDisc or allow metal or sharp surgical instruments to come in contact with the LapDisc as this may weaken or damage the flexible silicone membranes.
• Sterile, water-soluble lubricant should be applied to the dorsum of the gloved hand prior to insertion through the LapDisc. Unlubricated hands may cause significant friction and tear the device.
• Do not remove the hand with the iris valve closed as it may tear the device.
• Do not overtighten the iris valve.
• Use caution when opening the iris valve when the abdomen is insufflated, as rapid loss of pneumoperitoneum may occur.
• After removing the instrument, inspect the site for hemostasis. If hemostasis is not present, appropriate techniques should be used to achieve hemostasis.
• Instruments or devices which come into contact with bodily fluids may require special disposal handling to prevent biological contamination.
• Dispose of all opened instruments whether used or unused. Do not resterilize the instrument. Resterilization may compromise the integrity of the device which may result in unintended injury.
Future Prospect of HALS
There are general and specific limitations, awaiting multicenter prospective randomized trials in order to compare HALS in various major intra-abdominal procedures with the traditional open surgery. Hand-assisted laparoscopic surgery (HALS) can be used for all major complex abdominal surgeries like:
• Splenectomy
• Nephrectomy
• Morbid obesity surgery
• Pancreatectomy
• Nissen fundoplication
• Esophagectomy
• Rectopexy
• Repair of abdominal aortic aneurysm.
Hand-assisted laparoscopic surgery is technically much easier than total laparoscopy in advanced abdominal procedures. It can help the beginning laparoscopic surgeon to practice such major operations.
Hemicolectomy with HALS




