Laparoscopic Tayside Knot
The Tayside knot is safe for use with any braided material. It supplies a degree of resistance to reverse slippage equivalent to a surgeon's knot.
Step 1: A single hitch is taken first just as Roeder's knot.
Step 2: Four and a half rounds are taken approximately 1 cm below the first hitch over the long limb of thread.
Step 3: A locking hitch is made by passing the tail through the second and third loop.
Step 4: Finally the first hitch is brought closer to the locking hitch by spreading the first loop.
Step 5: The knot is stacked properly and the extra tail (if any) is cut. Once the knot is configured properly, it should be checked by sliding over the long thread.
Various step of Tayside knot:
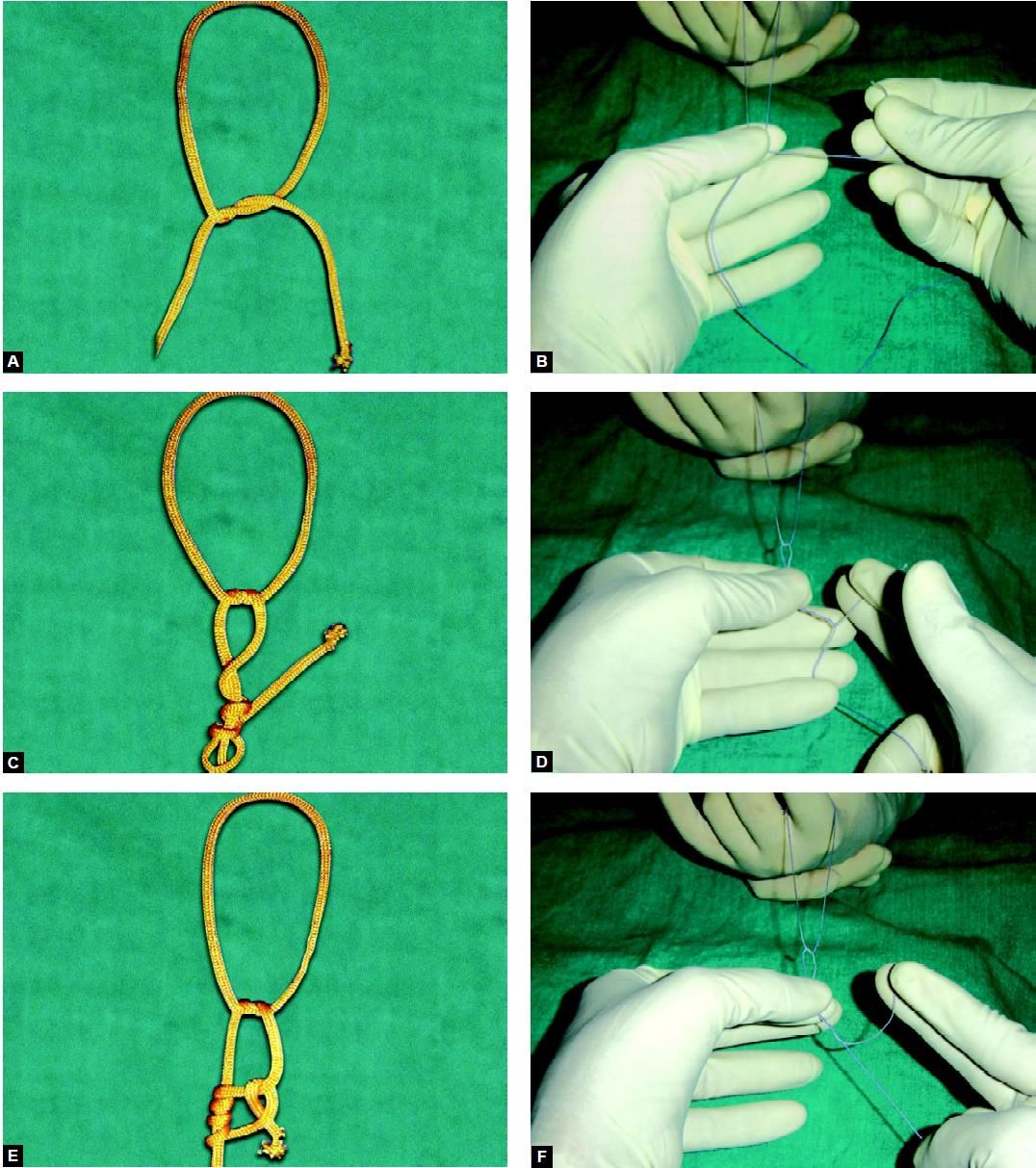
Steps A to F
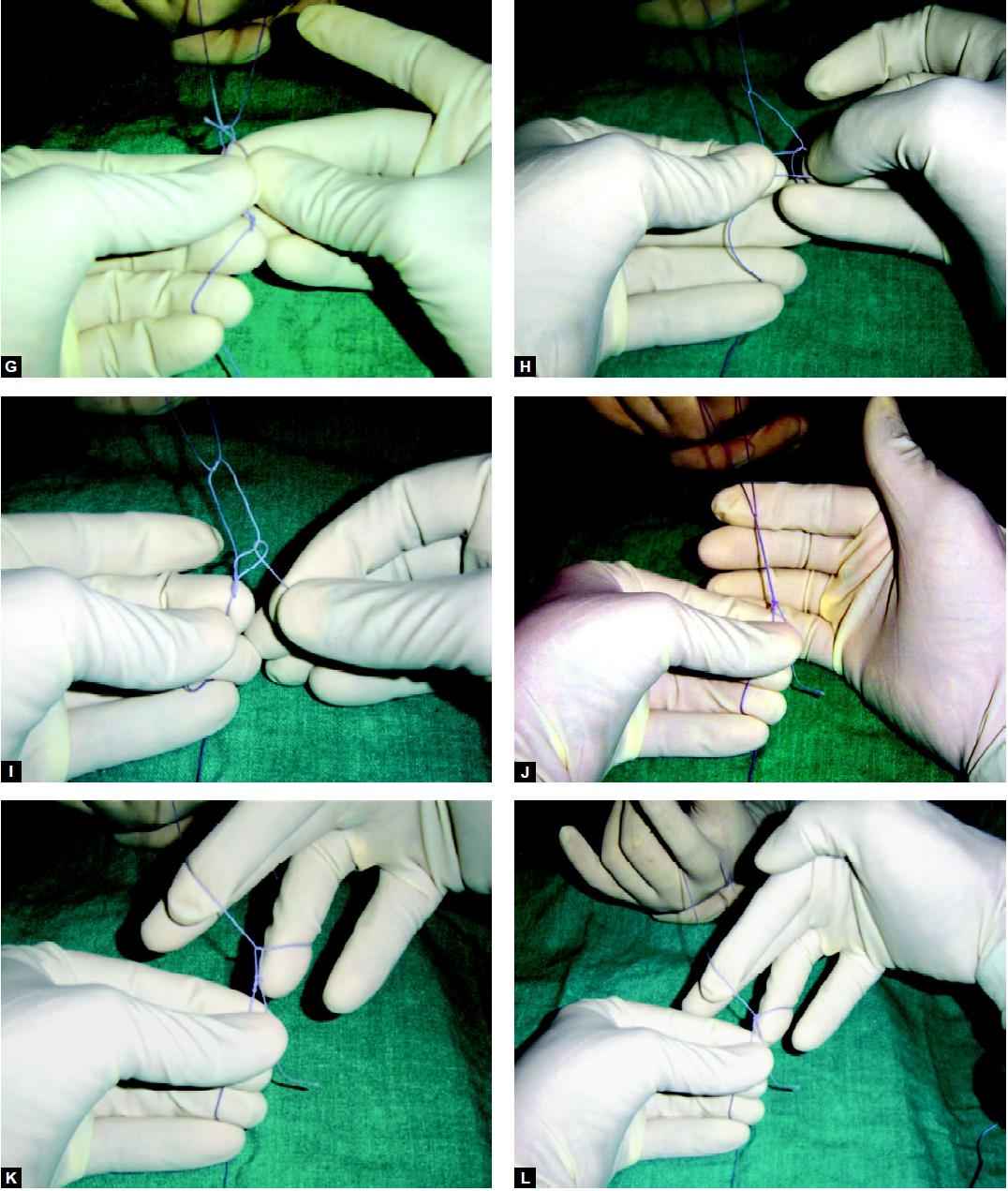
Steps G to L
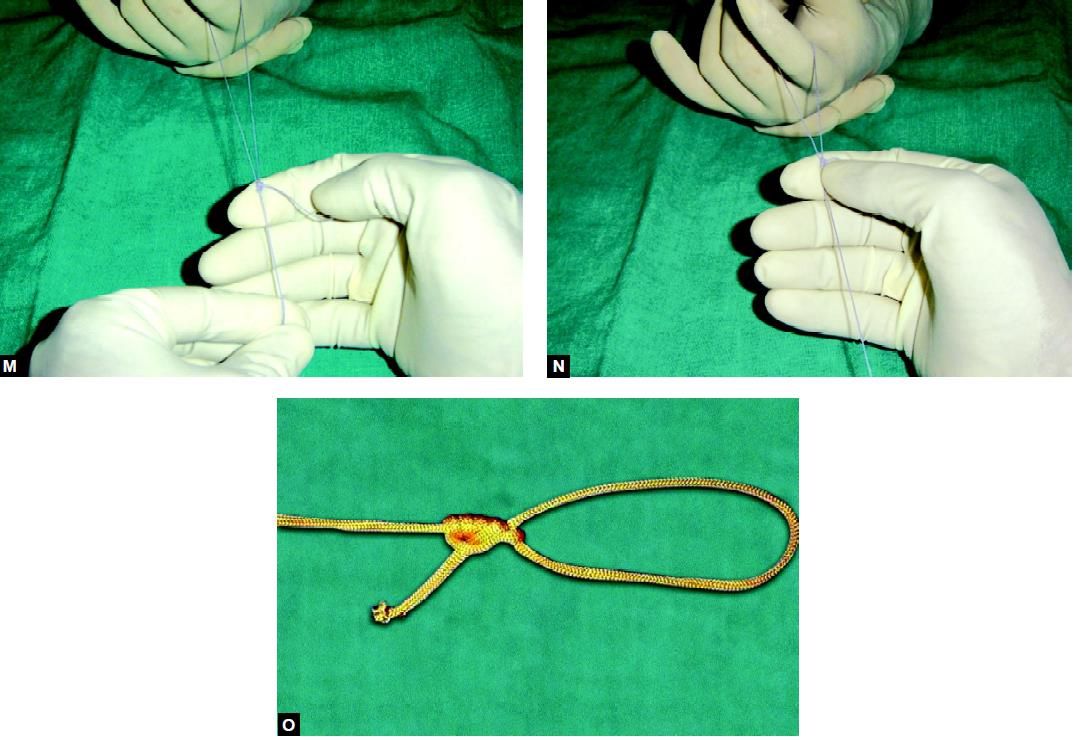
Steps M to O
Applications
The Tayside knot is suitable for use with all braided sutures (2/0 or stronger) as well as dacron. It is used with Dacron for ligation of vessels such as the azygous vein, splenic artery/ vein, or the inferior mesenteric artery/vein.
Using a Pretied Loop
• The loop is drawn up into the metal sleeve.
• The tube is then introduced through an abdominal port.
• Once inside the abdomen the loop is advanced using the pushrod.
• A grasping forceps is placed through the loop and used to grasp the tissue to be ligated.
• The loop is delivered over the tissue and the knot and push rod positioned at the base of the tissue.
• The loop is then tightened around the tissue by tensioning the long end and applying pressure to the knot via the push rod causing it to slide.
• The knot is locked firmly in place.
• The graspers are removed and replaced by suture scissors to divide the long end prior to removal.
Pretied loops are available commercially. They are packaged with the following items, assembled ready for use:
• A push rod
• A pretied loop
• A metal or silicon introducer tube.
The pretied loop has one long tail of suture material, which is threaded through the plastic pushrod and encapsulated by the end. The region at the end of the push rod is designed to be broken so the thread may be pulled through the remainder of the rod. The pushrod is passed through the metal introducer tube.
Clinical Uses
Preformed loops are used to ligate tissue, e.g. the base of the appendix, lung bullae, and a hole in the gall- bladder during cholecystectomy. If multiple loops are required, the pushrod and introducer can be reloaded with a length of ligature and additional loops fashioned by a surgeon with knowledge of external slip knots.
A preformed loop can also be used to secure a divided vessel after it has been isolated by a grasper. A slight modification of this technique allows it to be used to secure smaller identified vessels. One end is clipped and the other controlled by a grasper, which has already been passed through a loop. The vessel is divided and the loop slides into place and tightened before the grasper releases the vessel.
Endoloops are also useful for sealing a perforated organ if this is to be removed, e.g. perforation of the gallbladder during laparoscopic cholecystectomy where closure is necessary to prevent the escape of gallstones into the peritoneal cavity.
On no account must endoloops be used to close a perforation in any organ that is not going to be resected and removed, as the tissue included in the closed endoloop will slough off a few days later, because of ischemia, resulting in peritonitis.
Extracorporeal Knot for Continuous Structure
• A push rod is threaded onto a length of ligature material approximately 1.5 m long.
• A knot is tied at the end of the thread as it emerges from the straight end of the rod.
• The end of the ligature emerging from the tapered end is grasped by the atraumatic endoscopic grasper.
• The grasper and catgut are then passed into an introducer tube.
• The introducer tube is then passed through an 11 mm cannula.
• The grasper and ligature are extended into the cavity and passed to one side and behind the structure to be ligated.
• A second grasper is introduced through a second port to grasp the ligature from the other side of the structure.
• The first grasper releases the ligature and takes it back from the second in front of the structure.
• The first grasper and ligature are withdrawn from the abdomen through the introducer tube while the second is used to protect the structure from the suture.
• An external slip knot is tied externally. The knot tied is determined by the size of the vessel to be controlled and the material in use.
• The knot is pushed into the abdomen by the pushrod and positioned prior to tightening.
• The rod is withdrawn a little and scissors introduced to cut the thread leaving a reasonably long end.
The Tayside knot is safe for use with any braided material. It supplies a degree of resistance to reverse slippage equivalent to a surgeon's knot.
Step 1: A single hitch is taken first just as Roeder's knot.
Step 2: Four and a half rounds are taken approximately 1 cm below the first hitch over the long limb of thread.
Step 3: A locking hitch is made by passing the tail through the second and third loop.
Step 4: Finally the first hitch is brought closer to the locking hitch by spreading the first loop.
Step 5: The knot is stacked properly and the extra tail (if any) is cut. Once the knot is configured properly, it should be checked by sliding over the long thread.
Various step of Tayside knot:
Steps A to F
Steps G to L
Steps M to O
Applications
The Tayside knot is suitable for use with all braided sutures (2/0 or stronger) as well as dacron. It is used with Dacron for ligation of vessels such as the azygous vein, splenic artery/ vein, or the inferior mesenteric artery/vein.
Using a Pretied Loop
• The loop is drawn up into the metal sleeve.
• The tube is then introduced through an abdominal port.
• Once inside the abdomen the loop is advanced using the pushrod.
• A grasping forceps is placed through the loop and used to grasp the tissue to be ligated.
• The loop is delivered over the tissue and the knot and push rod positioned at the base of the tissue.
• The loop is then tightened around the tissue by tensioning the long end and applying pressure to the knot via the push rod causing it to slide.
• The knot is locked firmly in place.
• The graspers are removed and replaced by suture scissors to divide the long end prior to removal.
Pretied loops are available commercially. They are packaged with the following items, assembled ready for use:
• A push rod
• A pretied loop
• A metal or silicon introducer tube.
The pretied loop has one long tail of suture material, which is threaded through the plastic pushrod and encapsulated by the end. The region at the end of the push rod is designed to be broken so the thread may be pulled through the remainder of the rod. The pushrod is passed through the metal introducer tube.
Clinical Uses
Preformed loops are used to ligate tissue, e.g. the base of the appendix, lung bullae, and a hole in the gall- bladder during cholecystectomy. If multiple loops are required, the pushrod and introducer can be reloaded with a length of ligature and additional loops fashioned by a surgeon with knowledge of external slip knots.
A preformed loop can also be used to secure a divided vessel after it has been isolated by a grasper. A slight modification of this technique allows it to be used to secure smaller identified vessels. One end is clipped and the other controlled by a grasper, which has already been passed through a loop. The vessel is divided and the loop slides into place and tightened before the grasper releases the vessel.
Endoloops are also useful for sealing a perforated organ if this is to be removed, e.g. perforation of the gallbladder during laparoscopic cholecystectomy where closure is necessary to prevent the escape of gallstones into the peritoneal cavity.
On no account must endoloops be used to close a perforation in any organ that is not going to be resected and removed, as the tissue included in the closed endoloop will slough off a few days later, because of ischemia, resulting in peritonitis.
Extracorporeal Knot for Continuous Structure
• A push rod is threaded onto a length of ligature material approximately 1.5 m long.
• A knot is tied at the end of the thread as it emerges from the straight end of the rod.
• The end of the ligature emerging from the tapered end is grasped by the atraumatic endoscopic grasper.
• The grasper and catgut are then passed into an introducer tube.
• The introducer tube is then passed through an 11 mm cannula.
• The grasper and ligature are extended into the cavity and passed to one side and behind the structure to be ligated.
• A second grasper is introduced through a second port to grasp the ligature from the other side of the structure.
• The first grasper releases the ligature and takes it back from the second in front of the structure.
• The first grasper and ligature are withdrawn from the abdomen through the introducer tube while the second is used to protect the structure from the suture.
• An external slip knot is tied externally. The knot tied is determined by the size of the vessel to be controlled and the material in use.
• The knot is pushed into the abdomen by the pushrod and positioned prior to tightening.
• The rod is withdrawn a little and scissors introduced to cut the thread leaving a reasonably long end.


