Use of Electrosurgical Hooks in Laparoscopic Surgery
These are generally L or open C shaped, blunt-ended rods mounted on an insulated handle. The active, non-insulated part is limited in size. The hook is a delicate instrument and should be protected during insertion by the manual opening of the cannula valve or the use of a reducing tube. As electrosurgery generates smoke (which is harmful), many handles of electrosurgical hooks have a suction attachment at the other end of the handle.
Electrosurgical Hooks
Electrosurgical instruments like the hook are useful as blunt dissectors prior to activation. They are used to isolate the tissue to be divided by the current. The tip is passed into or under a layer of the tissue being dissected, which is then hooked and tented up (to increase its impedance and thus limit the spread of current when applied). Small portions of tissue are tackled so that an assessment of the tissue caught on the hook can be made before coagulation or cutting current is applied to the instrument. The hook can be used to clear unwanted tissue beside linear structures by passing the hook into the tissues parallel to the structure, and then rotating it to hook up strands of unwanted tissue. The tissue to be divided is held away from underlying tissue to prevent inadvertent damage. Short bursts of coagulating current can be followed by the use of cutting current if the tissue has not already separated. The use of the hook can be summarized as “hook, look, cook”.
The hook or the spatula may be used to mark out and coagulate a line for the division. The heel of the hook is used with the HF current set to soft coagulation. Short bursts are applied and the hook moved along to create a “dotted” line of coagulated tissue. When deeper penetration is desired, the hook is an appropriate instrument. This type of contact is best reserved for a situation where no significant damage can be caused by current penetration.
Monopolar electrosurgery has become the most widely used cutting and coagulating technique in minimal access surgery. It has proven to be versatile, cost-effective, and demonstrated superior efficacy for coagulation. By varying the voltage, current or waveform, tissue can be cut cleanly (pure cut); coagulated to achieve hemostasis (coag mode) or a “blend cut” that combines these two functions can also be produced. Finally, a dispersed coagulation mode known as fulguration allows the coagulation of diffuse bleeding.

Different types of hook
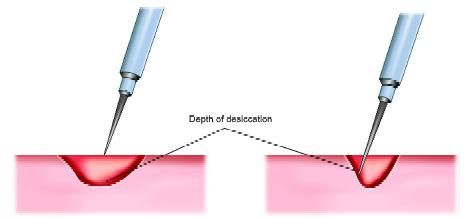
Depth of desiccation is proportional to paddle application time
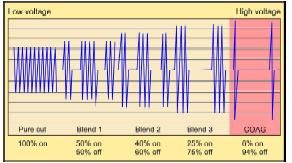
Different types of electrosurgery
Cutting current is low voltage high-frequency current. Due to high frequency, the ions inside the cell get turbulence and cell burst (explode or vaporize). Cutting current can be obtained by pressing the yellow paddle of the electrosurgical generator. To cut any structure it is important that the surgeon should apply the sharp tip of the electrosurgical instrument and the tissue should not be held firmly. At the time of cutting it is wise that tissue should be under tension. Ideally, direct touch with the tissue should be avoided in case of cutting current. It should be a spark wave from some distance.
Electrosurgical coagulation is achieved by high voltage low-frequency current. This low frequency is not sufficient to cause the explosion of a cell but the heat inside the cell is increased. Due to increased intracellular temperature, the protein inside the cell coagulates and shrinks. Shrinkage of protein will cause constriction in the lumen of bleeding vessels and the vessels are sealed. Permanency of coagulated tissue and its sealing effect depends upon melted collagen. At the time of electrosurgical monopolar coagulation the temperature of tissue cause the collagen to melt. These melted collagens solidify again once the active instrument is off from the tissue. It is important to remember that if the tissue is burnt more than required, the melted collagen burns, turns into charcoal and the sealing strength of the lumen of any vessel will decrease. Surgeons and gynecologists should always try to avoid overcooking of the tissue.
Electrosurgical coagulation is of two types:
Fulguration
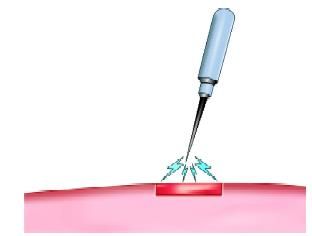
Fulguration is coagulation current from some distance. It is also known as spray mode. At the time of fulguration lateral spread of energy is more than depth. We want to use fulguration everywhere, where the superficial burn is required and deeper injury may cause damage to the underlying structure. The example of good use fulguration is ablation in cases of endometriosis, fulguration of gallbladder bed at the time of cholecystectomy if there is generalized oozing from the liver. Direct touch with tissue should be avoided to achieve maximum effect. Fulguration is coagulation current from some distance.
Fulguration
Desiccation
Electrosurgical desiccation occurs when the electrode is in direct contact with the tissue. Most of the time with the unipolar or bipolar electrosurgery we do desiccation only. The tissue damage in-depth and width is the same in desiccation. The extent of collateral damage in desiccation is more compared to cutting current. The extent of the collateral damage of desiccation can be minimized by minimizing the paddle application time.

Desiccation with more collateral damage

Desiccation with less collateral damage
However, monopolar laparoscopic electrosurgery can compromise patient safety under certain circumstances. Thermal injury to nontargeted internal organs may occur firstly, as a result of the imprecise mechanical operation of a laparoscopic instrument and secondly, through the diversion of electrical current to other paths. These stray current may be released either through insulation failure, direct coupling or capacitive coupling. Other problems encountered include effect on pacemakers; return electrode burns, toxic smoke, charring of instruments, and minimal control of energy delivery.
Bipolar electrodes design although virtually eliminating complications from insulation failure, capacitive coupling, and direct coupling. The primary electrothermal tissue effect is limited to desiccation, not cutting. It requires slightly more time than monopolar coagulation because of lower power settings and bipolar generator output characteristics. It is not an effective method of making a “pure cut”.
• Hemostasis over a large area is not possible
• Grasping dense tissue between both the active and return electrodes is difficult.

Overshooting should be avoided
These are generally L or open C shaped, blunt-ended rods mounted on an insulated handle. The active, non-insulated part is limited in size. The hook is a delicate instrument and should be protected during insertion by the manual opening of the cannula valve or the use of a reducing tube. As electrosurgery generates smoke (which is harmful), many handles of electrosurgical hooks have a suction attachment at the other end of the handle.
Electrosurgical Hooks
Electrosurgical instruments like the hook are useful as blunt dissectors prior to activation. They are used to isolate the tissue to be divided by the current. The tip is passed into or under a layer of the tissue being dissected, which is then hooked and tented up (to increase its impedance and thus limit the spread of current when applied). Small portions of tissue are tackled so that an assessment of the tissue caught on the hook can be made before coagulation or cutting current is applied to the instrument. The hook can be used to clear unwanted tissue beside linear structures by passing the hook into the tissues parallel to the structure, and then rotating it to hook up strands of unwanted tissue. The tissue to be divided is held away from underlying tissue to prevent inadvertent damage. Short bursts of coagulating current can be followed by the use of cutting current if the tissue has not already separated. The use of the hook can be summarized as “hook, look, cook”.
The hook or the spatula may be used to mark out and coagulate a line for the division. The heel of the hook is used with the HF current set to soft coagulation. Short bursts are applied and the hook moved along to create a “dotted” line of coagulated tissue. When deeper penetration is desired, the hook is an appropriate instrument. This type of contact is best reserved for a situation where no significant damage can be caused by current penetration.
Monopolar electrosurgery has become the most widely used cutting and coagulating technique in minimal access surgery. It has proven to be versatile, cost-effective, and demonstrated superior efficacy for coagulation. By varying the voltage, current or waveform, tissue can be cut cleanly (pure cut); coagulated to achieve hemostasis (coag mode) or a “blend cut” that combines these two functions can also be produced. Finally, a dispersed coagulation mode known as fulguration allows the coagulation of diffuse bleeding.
Different types of hook
Depth of desiccation is proportional to paddle application time
Different types of electrosurgery
Cutting current is low voltage high-frequency current. Due to high frequency, the ions inside the cell get turbulence and cell burst (explode or vaporize). Cutting current can be obtained by pressing the yellow paddle of the electrosurgical generator. To cut any structure it is important that the surgeon should apply the sharp tip of the electrosurgical instrument and the tissue should not be held firmly. At the time of cutting it is wise that tissue should be under tension. Ideally, direct touch with the tissue should be avoided in case of cutting current. It should be a spark wave from some distance.
Electrosurgical coagulation is achieved by high voltage low-frequency current. This low frequency is not sufficient to cause the explosion of a cell but the heat inside the cell is increased. Due to increased intracellular temperature, the protein inside the cell coagulates and shrinks. Shrinkage of protein will cause constriction in the lumen of bleeding vessels and the vessels are sealed. Permanency of coagulated tissue and its sealing effect depends upon melted collagen. At the time of electrosurgical monopolar coagulation the temperature of tissue cause the collagen to melt. These melted collagens solidify again once the active instrument is off from the tissue. It is important to remember that if the tissue is burnt more than required, the melted collagen burns, turns into charcoal and the sealing strength of the lumen of any vessel will decrease. Surgeons and gynecologists should always try to avoid overcooking of the tissue.
Electrosurgical coagulation is of two types:
Fulguration
Fulguration is coagulation current from some distance. It is also known as spray mode. At the time of fulguration lateral spread of energy is more than depth. We want to use fulguration everywhere, where the superficial burn is required and deeper injury may cause damage to the underlying structure. The example of good use fulguration is ablation in cases of endometriosis, fulguration of gallbladder bed at the time of cholecystectomy if there is generalized oozing from the liver. Direct touch with tissue should be avoided to achieve maximum effect. Fulguration is coagulation current from some distance.
Fulguration
Desiccation
Electrosurgical desiccation occurs when the electrode is in direct contact with the tissue. Most of the time with the unipolar or bipolar electrosurgery we do desiccation only. The tissue damage in-depth and width is the same in desiccation. The extent of collateral damage in desiccation is more compared to cutting current. The extent of the collateral damage of desiccation can be minimized by minimizing the paddle application time.
Desiccation with more collateral damage
Desiccation with less collateral damage
However, monopolar laparoscopic electrosurgery can compromise patient safety under certain circumstances. Thermal injury to nontargeted internal organs may occur firstly, as a result of the imprecise mechanical operation of a laparoscopic instrument and secondly, through the diversion of electrical current to other paths. These stray current may be released either through insulation failure, direct coupling or capacitive coupling. Other problems encountered include effect on pacemakers; return electrode burns, toxic smoke, charring of instruments, and minimal control of energy delivery.
Bipolar electrodes design although virtually eliminating complications from insulation failure, capacitive coupling, and direct coupling. The primary electrothermal tissue effect is limited to desiccation, not cutting. It requires slightly more time than monopolar coagulation because of lower power settings and bipolar generator output characteristics. It is not an effective method of making a “pure cut”.
• Hemostasis over a large area is not possible
• Grasping dense tissue between both the active and return electrodes is difficult.
Overshooting should be avoided





