High-Frequency Electrosurgical Dissection
Our household appliances have the 50 to 60 Hz frequency. This frequency is beneficial because if a faulty instrument has current and inadvertently someone touches, then he will be thrown away and the person getting shocked will be safe. If the frequency is more than 100 kHz, muscle and nerve stimulation ceases, whereas, all other property of the electric current is still there. High-frequency electrosurgery is the application of high frequency (HF) currents (in the frequency range of 300 kHz up to several MHz) to coagulate, fulgurate, spray coagulates or ablates tissue. Knowledge of how this and other physical modes interact with biological materials is becoming increasingly important to the surgeon for safe and consistent surgery.
• Standard electrical current alternates at a frequency of 50 cycles per second (Hz).
• Nerve and muscle stimulation cease at 100,000 cycles/ second (100 kHz).
• Electrosurgery can be performed safely at frequencies above 100 kHz.
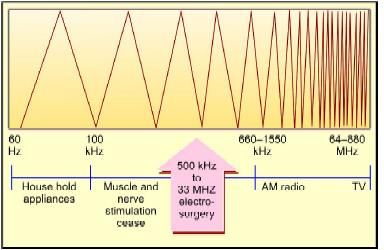
The frequency range of electrosurgery
HF Monopolar Electrosurgery
The monopolar circuit is composed of the generator, active electrode, patient, and patient return electrode. The patient's tissue provides resistance, producing heat. Monopolar diathermy is used in endoscopic surgery for coagulation and for dissection (cutting). During monopolar diathermy, a current is conducted from the instrument through the tissues to a skin pad (neutral electrode) connected back to the generator. Heating occurs at the site of small cross-section and low electrical conductivity. A high current density occurs in the tissue in immediate contact with the instrument and heat is generated.
Burn = Intensity of current × Time/area
The burn is directly proportional to the intensity of the current. The intensity of the current can be adjusted by the knob provided in the generator's control panel. If the intensity setting is more the burn will be more. Intensity actually denotes ampere or number of electrons that flow through the pathway.
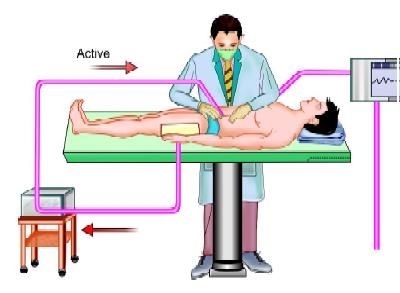
Circuit of monopolar current
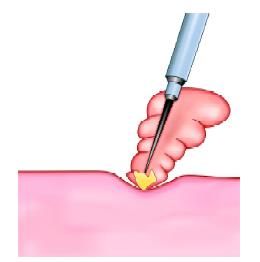
The burn is also directly proportional to time. Time is a paddle application time. The surgeon should always keep in mind that continuous activation of paddle can result in many complications. Intermittent activation is always better than continuous activation. The burn is inversely proportional to the area. One of the major problems in electrosurgery is patient will get burn at the site where the area is narrowest. This may cause remote injury with the use of monopolar diathermy. The surgeon should hold the tissue with the point of the instrument to catch the minimum amount of tissue at one time. If a bunch of tissue is caught there is always the fear of remote injury.
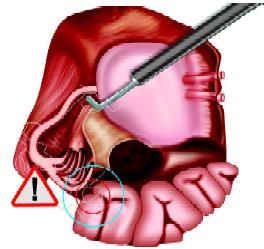
Remote injury
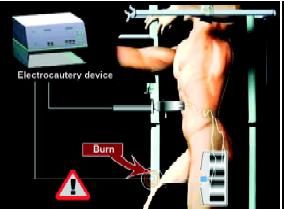
Remote injury with an electrocautery device
Patient Return Electrodes
Silicon and metal patient return plates are available. The silicon is better because it does not have any sharp edge and the resistance is less. The patient return electrode is required only in unipolar electrosurgery because the patient's body is a part of the circuit and the patient return plate will take the current back to the generator. If the patient return plate is not attached properly to the body of the patient, or the size of the patient return plate is very small, the patient can get an electric burn at the point of attachment of this patient return plate. Ideally, the size of patient return plate should not be less than 100 cm2. At the time of the location of the patient return, plate attachment surgeon should keep in mind the following points.

Silicon plate
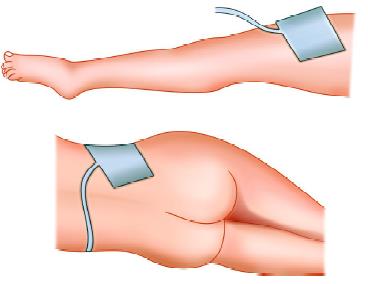
Patient return plate
Choose
Well vascularized muscle mass to have more area of contact.
Avoid
• Vascular insufficiency should be avoided because of high resistant
• Irregular body contours can prevent plate to be in firm contact
• Bony prominences will not allow the surrounding skin to be in contact.
Consider
• Plate should be nearer to the incision site
• Plate should be placed according to patients position so should not be displaced
• Plate should be away from other equipments like cardiac monitor.
The effect of HF current on the tissues depends on:
• Temperature generated.
• Shape and dimensions of the contact point (broader damage with broader contact)
• Time of activation (short bursts reduce depth and charring)
• Distance from the electrode
• Conductivity of the tissue (bleeding results in a change in conductivity)
• Power output from the generator (voltage)
• Amplitude and current waveform time curve of the signal (cutting or coagulating settings).
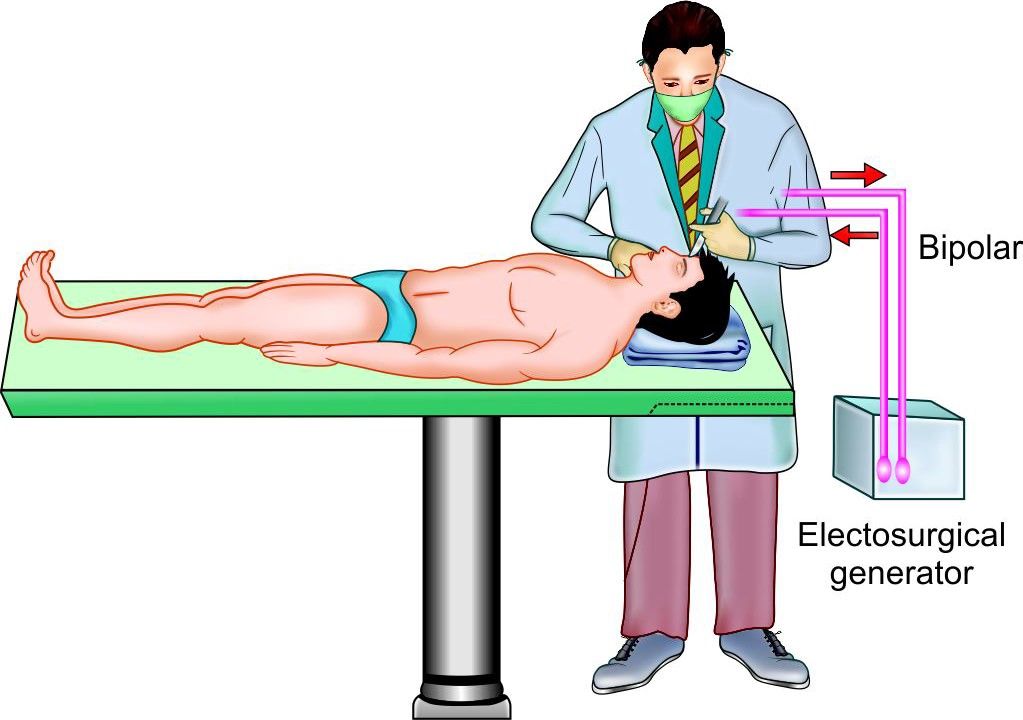
Bipolar Diathermy
A bipolar system is inherently safer as the interaction is restricted to the immediate vicinity of contact and the current does not pass through the patient but instead returns to the generator via the receiving pole after passage through the grasped tissue.
Bipolar Electrosurgery
• Active output and patient return functions are both are at the site of surgery.
• The Current path is confined to tissue grasped between forceps.
• Return electrode should not be applied for bipolar procedures.
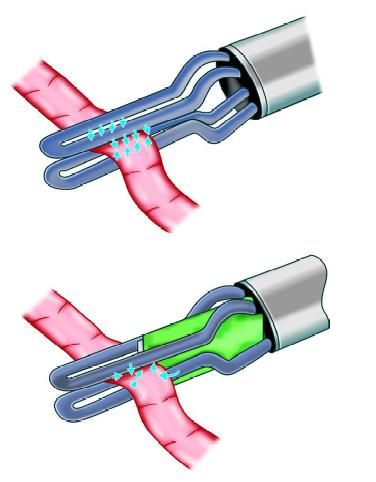
Effect of cutting current
Circuit of bipolar current

Bipolar forceps used in LAVH
Tripolar Electrosurgery
Bipolar probes are now available for coagulation as well as for cutting. The cutting system is not strictly bipolar and is hence referred to as tripolar.
It has four functions in one and the same instrument namely:
1. Dissecting
2. Grasping
3. Bipolar coagulation
4. Bipolar cut.
Tripolar device
Our household appliances have the 50 to 60 Hz frequency. This frequency is beneficial because if a faulty instrument has current and inadvertently someone touches, then he will be thrown away and the person getting shocked will be safe. If the frequency is more than 100 kHz, muscle and nerve stimulation ceases, whereas, all other property of the electric current is still there. High-frequency electrosurgery is the application of high frequency (HF) currents (in the frequency range of 300 kHz up to several MHz) to coagulate, fulgurate, spray coagulates or ablates tissue. Knowledge of how this and other physical modes interact with biological materials is becoming increasingly important to the surgeon for safe and consistent surgery.
• Standard electrical current alternates at a frequency of 50 cycles per second (Hz).
• Nerve and muscle stimulation cease at 100,000 cycles/ second (100 kHz).
• Electrosurgery can be performed safely at frequencies above 100 kHz.
The frequency range of electrosurgery
HF Monopolar Electrosurgery
The monopolar circuit is composed of the generator, active electrode, patient, and patient return electrode. The patient's tissue provides resistance, producing heat. Monopolar diathermy is used in endoscopic surgery for coagulation and for dissection (cutting). During monopolar diathermy, a current is conducted from the instrument through the tissues to a skin pad (neutral electrode) connected back to the generator. Heating occurs at the site of small cross-section and low electrical conductivity. A high current density occurs in the tissue in immediate contact with the instrument and heat is generated.
Burn = Intensity of current × Time/area
The burn is directly proportional to the intensity of the current. The intensity of the current can be adjusted by the knob provided in the generator's control panel. If the intensity setting is more the burn will be more. Intensity actually denotes ampere or number of electrons that flow through the pathway.
Circuit of monopolar current
The burn is also directly proportional to time. Time is a paddle application time. The surgeon should always keep in mind that continuous activation of paddle can result in many complications. Intermittent activation is always better than continuous activation. The burn is inversely proportional to the area. One of the major problems in electrosurgery is patient will get burn at the site where the area is narrowest. This may cause remote injury with the use of monopolar diathermy. The surgeon should hold the tissue with the point of the instrument to catch the minimum amount of tissue at one time. If a bunch of tissue is caught there is always the fear of remote injury.
Remote injury
Remote injury with an electrocautery device
Patient Return Electrodes
Silicon and metal patient return plates are available. The silicon is better because it does not have any sharp edge and the resistance is less. The patient return electrode is required only in unipolar electrosurgery because the patient's body is a part of the circuit and the patient return plate will take the current back to the generator. If the patient return plate is not attached properly to the body of the patient, or the size of the patient return plate is very small, the patient can get an electric burn at the point of attachment of this patient return plate. Ideally, the size of patient return plate should not be less than 100 cm2. At the time of the location of the patient return, plate attachment surgeon should keep in mind the following points.
Silicon plate
Patient return plate
Choose
Well vascularized muscle mass to have more area of contact.
Avoid
• Vascular insufficiency should be avoided because of high resistant
• Irregular body contours can prevent plate to be in firm contact
• Bony prominences will not allow the surrounding skin to be in contact.
Consider
• Plate should be nearer to the incision site
• Plate should be placed according to patients position so should not be displaced
• Plate should be away from other equipments like cardiac monitor.
The effect of HF current on the tissues depends on:
• Temperature generated.
• Shape and dimensions of the contact point (broader damage with broader contact)
• Time of activation (short bursts reduce depth and charring)
• Distance from the electrode
• Conductivity of the tissue (bleeding results in a change in conductivity)
• Power output from the generator (voltage)
• Amplitude and current waveform time curve of the signal (cutting or coagulating settings).
Bipolar Diathermy
A bipolar system is inherently safer as the interaction is restricted to the immediate vicinity of contact and the current does not pass through the patient but instead returns to the generator via the receiving pole after passage through the grasped tissue.
Bipolar Electrosurgery
• Active output and patient return functions are both are at the site of surgery.
• The Current path is confined to tissue grasped between forceps.
• Return electrode should not be applied for bipolar procedures.
Effect of cutting current
Circuit of bipolar current
Bipolar forceps used in LAVH
Tripolar Electrosurgery
Bipolar probes are now available for coagulation as well as for cutting. The cutting system is not strictly bipolar and is hence referred to as tripolar.
It has four functions in one and the same instrument namely:
1. Dissecting
2. Grasping
3. Bipolar coagulation
4. Bipolar cut.
Tripolar device




