Principle of Laparoscopic Port Position
The relative position of the instrument ports is very important in the performance of surgical procedures endoscopically. The angle the instruments make with the operative site and to each other should mimic, as far as possible to the natural relationship of the hands and eyes during conventional surgery. It is proved that the most common cause of stressful minimal access surgery is the wrong port position. The umbilicus commonly is selected as the site for primary trocar insertion because it offers the shortest distance between the skin and the anterior peritoneum and is cosmetically appealing.
There are different sites of the primary optical port in laparoscopic surgery.
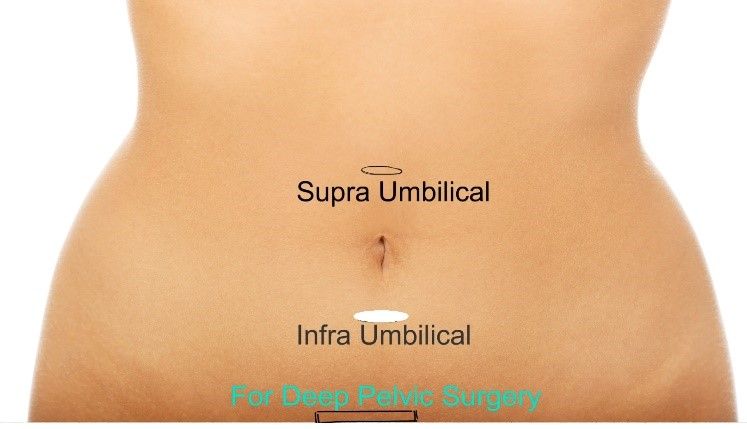
1. Supra Umbilical
2. Umbilical
a. Superior Crease of Umbilicus
b. Inferior Crease of Umbilicus
c. Trans Umbilical
3. Infra Umbilical
4. Palmer’s Point
Infra Umbilical Port
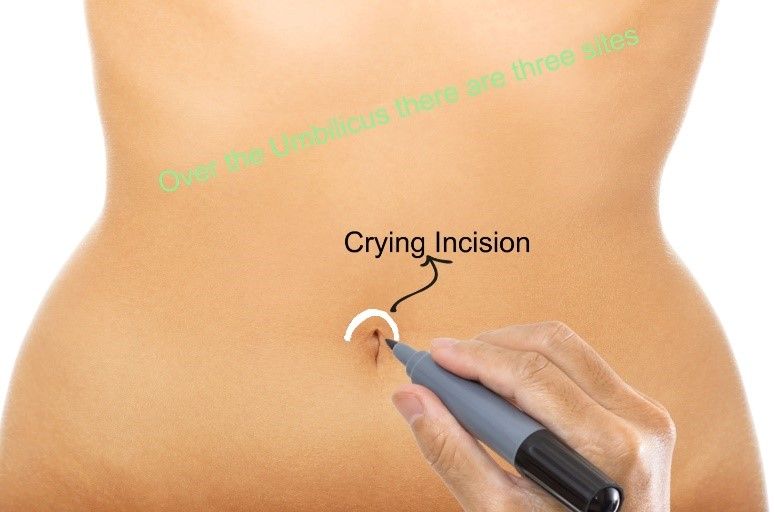
Superior Crease of Umbilicus
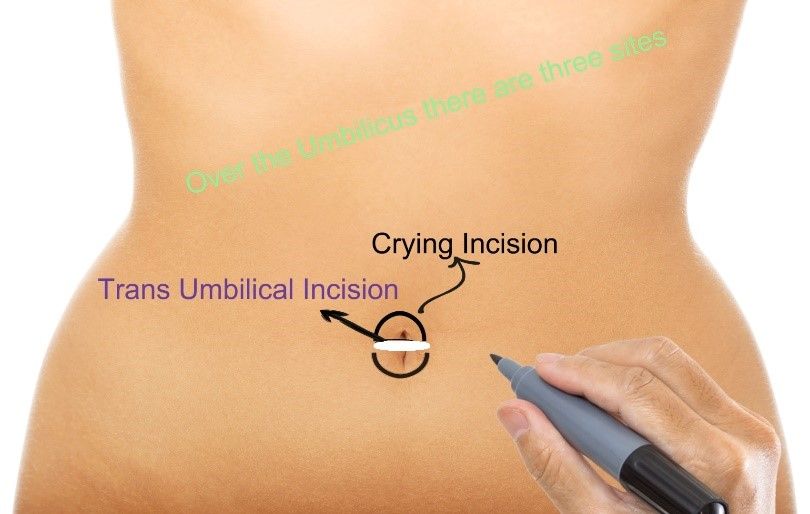
Trans Umbilical Port
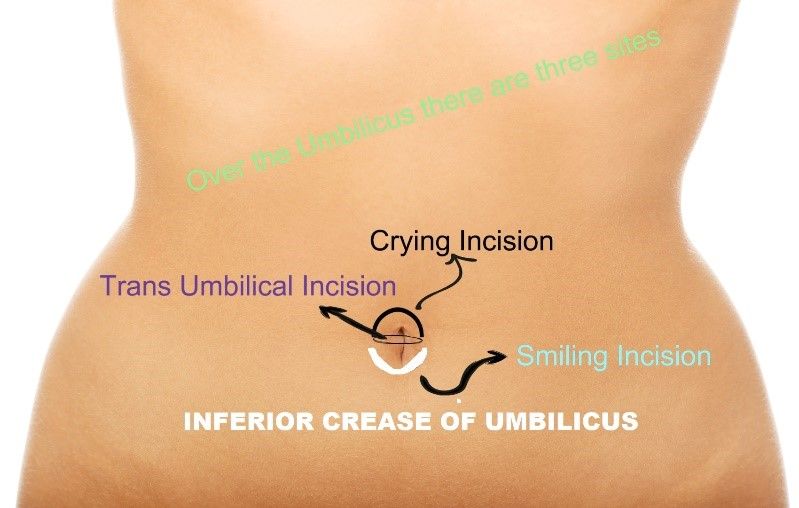
Inferior Crease of Umbilicus
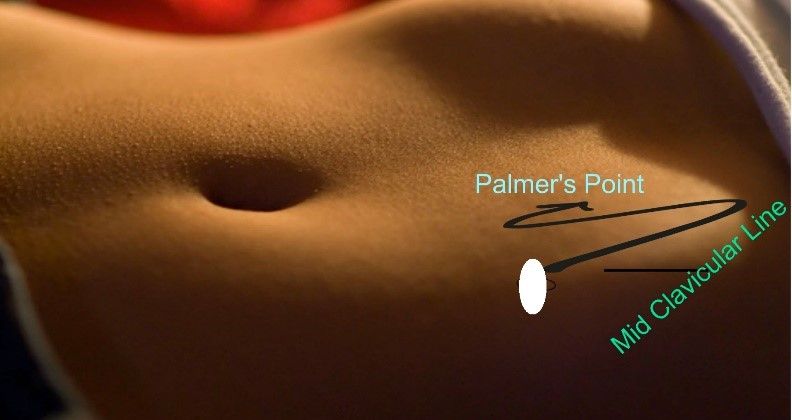
Palmer’s Point
SupraumbilicalPort Position
Despite its common use and its relation to vital abdominal structures, there are often in gynecology when an umbilical port is not ergonomically optimum. Supraumbilical primary trocar is highly advantageous for upper abdominal surgery like fundoplication heller’s myotomy, hiatus hernia, and most of the bariatric surgery. It is also an optimum port position for most of the gynecological surgery. Advances in laparoscopy have demonstrated that supraumbilical primary ports can be desirable in complex cases with large masses. It helps to increase the distance from enlarged pelvic pathology and thereby improve exposure and surgical efficiency. Supraumbilical port use has been reported in the literature to enable minimally invasive surgical management of large fibroid uteri at the time of myomectomy or hysterectomy and of large ovarian cyst. This port position is also useful in pregnant patients with the gravid uterus. In these instances, creating distance between the primary trocar and the uterus is especially important to avoid any penetrating injury to the gravid uterus from trocar insertion. Supraumbilical port use is also reported in the literature by gynecologic oncologists for laparoscopic excision of large ovarian cancers. The supraumbilical primary port is also frequently used in robotic surgery when increased inter port distances are desirable to eliminate robotic arm collisions. Reports in the literature describe the common locations of the supraumbilical port site are 5 cm above the umbilicus and at least 6 to 10 cm above a second-trimester gravid uterus or very large uterus and ovarian cyst. In an obese patient where umbilicus is displaced down, xiphisternum should be used to plan supraumbilical port. For upper abdominal surgery and most of the bariatric surgery, supraumbilical port incisions should be given 18cm below the xiphisternum.
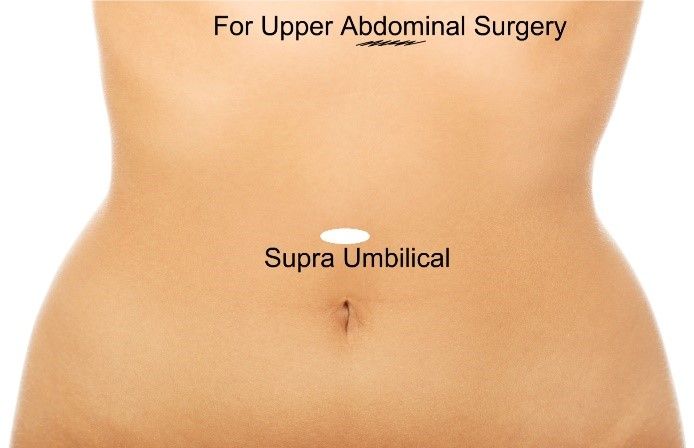
Supra Umbilical Port
Infraumbilical Port
This port position is less commonly used in laparoscopic surgery. Infraumbilical port is used 3-5 cm below the umbilicus. Infraumbilical port should not be confused with the port of the inferior crease of umbilicus. This port position is used in the following surgery:
1. Single puncture sterilization
2. For upper abdominal surgery (Cholecystectomy or Duodenal Perforation) in very small height patients.
Primary Port Position
The central location and ability of the umbilicus to camouflage scars make it an attractive primary port site for laparoscopic surgery. There are many drawbacks to the umbilicus as well. The umbilicus is a naturally weak area due to the absence of all the layers. Weakness is also due to its location at the midpoint of the abdomen’s greatest diameter.
It is easy to believe that there is a difference between the umbilicus and other trocar sites in both susceptibilities to infection and postoperative incisional herniation.
The study showed that the increased infection rate at the umbilicus seems to be related to the retrieval of infected organs through the umbilicus and not to the umbilicus itself. When umbilicus was used to retrieve gallbladder after cholecystectomy the rate of infection was high due to port contamination with the infected gallbladder. Excluding cholecystectomy, the umbilical infection rate was two percent, similar to that of any alternative site. The postoperative ventral hernia rate was at 0.8 percent, the same at the umbilicus as elsewhere if the port more than 10 mm size is not repaired. It is now proved that the wound infection at the umbilicus is similar to that at other sites; postoperative ventral hernia at the umbilicus is similar to that at other sites and most of the infection after laparoscopic cholecystectomy is due to the contamination of wound due to infected gallbladder.
Secondary Port Position
The obligatory passage of the laparoscopic instruments through the abdominal wall generates a fixed point after which all movements are reversed. For instance, when the hand moves to the left, the end of the instrument moves right, and when the hand moves downwards, the end of the instrument moves upwards. For some surgeons, the fulcrum effect is not a problem, but for others, it is an insurmountable obstacle to the performance of advanced laparoscopy.
Because the handling of laparoscopic instruments is through the fixed point at the abdominal wall, the force feedback felt by the surgeon will depend on the length of the instrument inferior to this fixed point.
Baseball Diamond Concept of Port Position
A satisfactory relationship includes:
• An angle of 60° between the two instrument tips
• Tangential approach to the site
• Appropriate working distance
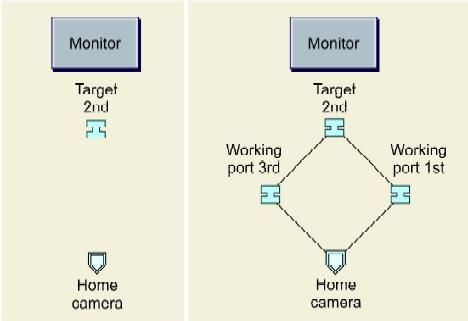
Baseball diamond concept of port position
First, decide the Target
Target may be in the suprapubic region for LAVH, right iliac fossa for appendicectomy, right upper quadrant for laparoscopic cholecystectomy, or left upper quadrant for fundoplication.

First, decide the target
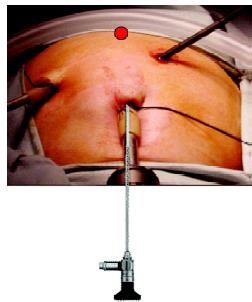
Draw the Line of Optimum Area
For optimum task performance, half to the two-third instrument should be inside the abdomen. The size of the adult laparoscopic instrument is 36 cm and the pediatrics instrument is 28 cm.
Telescope and Instruments
• Telescope should be in the middle of the working instrument.
The telescope should be in the center of the working instrument
• Manipulation angle of instruments should be 60 degrees.
Manipulation angle 60° is the angle between tips of the instrument
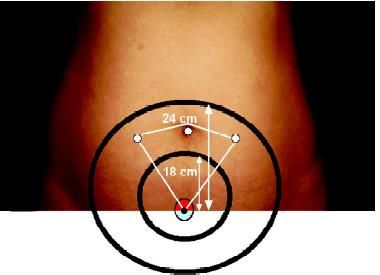
Rule of Diamond for LAVH
These factors combined with the specific anatomy will determine individual port sites. For standard operations like cholecystectomy, standard port sites related to surface marking may suffice but as more advanced or varied situations are tackled we recommend that you master the skill of individual port placement using the internal view. In general, the optic and the two main operating ports usually lie at the points of a flattened triangle, the optic being centrally and more distally placed. Try to keep ports at least 5 cm apart.
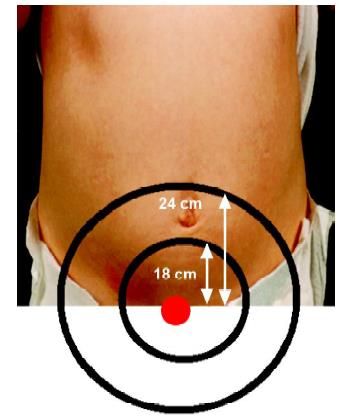
Draw two arcs on the abdominal wall at 18 and 24 cm from that point and note area in between

Measure the length of the instrument
Manipulation angle 60° is essential for optimum task performance in laparoscopic surgery.
Drawbacks of Incorrect Port Position
Swording
Swording occurs when the telescope or the shaft of the assistant’s instrument obstructs the operator’s instruments. If this occurs you may need to consider:
• Repositioning retracting instruments
• Rotation of an angled telescope allowing alteration of the position of the end of the telescope
• Withdrawal of the telescope
• Transposition of the operator’s instruments
• Additional port placement
• Changing the instruments to a different port.
Port Positions
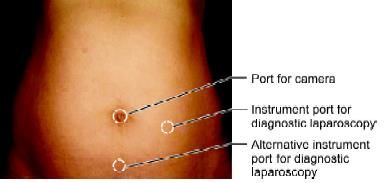
Port position for diagnostic laparoscopy
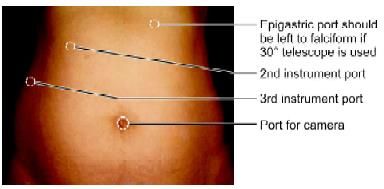
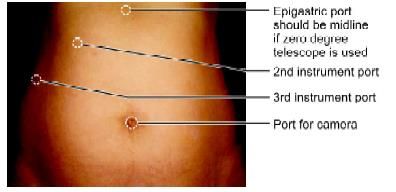
Port position for cholecystectomy
Alternative port position for cholecystectomy
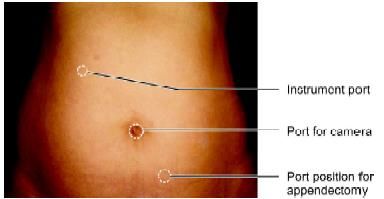
Port position for appendectomy
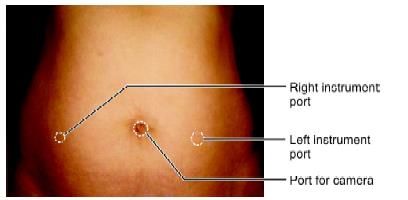
Position for bilateral hernia, LAVH and most of the gynecological procedures
The relative position of the instrument ports is very important in the performance of surgical procedures endoscopically. The angle the instruments make with the operative site and to each other should mimic, as far as possible to the natural relationship of the hands and eyes during conventional surgery. It is proved that the most common cause of stressful minimal access surgery is the wrong port position. The umbilicus commonly is selected as the site for primary trocar insertion because it offers the shortest distance between the skin and the anterior peritoneum and is cosmetically appealing.
There are different sites of the primary optical port in laparoscopic surgery.
1. Supra Umbilical
2. Umbilical
a. Superior Crease of Umbilicus
b. Inferior Crease of Umbilicus
c. Trans Umbilical
3. Infra Umbilical
4. Palmer’s Point
Infra Umbilical Port
Superior Crease of Umbilicus
Trans Umbilical Port
Inferior Crease of Umbilicus
Palmer’s Point
SupraumbilicalPort Position
Despite its common use and its relation to vital abdominal structures, there are often in gynecology when an umbilical port is not ergonomically optimum. Supraumbilical primary trocar is highly advantageous for upper abdominal surgery like fundoplication heller’s myotomy, hiatus hernia, and most of the bariatric surgery. It is also an optimum port position for most of the gynecological surgery. Advances in laparoscopy have demonstrated that supraumbilical primary ports can be desirable in complex cases with large masses. It helps to increase the distance from enlarged pelvic pathology and thereby improve exposure and surgical efficiency. Supraumbilical port use has been reported in the literature to enable minimally invasive surgical management of large fibroid uteri at the time of myomectomy or hysterectomy and of large ovarian cyst. This port position is also useful in pregnant patients with the gravid uterus. In these instances, creating distance between the primary trocar and the uterus is especially important to avoid any penetrating injury to the gravid uterus from trocar insertion. Supraumbilical port use is also reported in the literature by gynecologic oncologists for laparoscopic excision of large ovarian cancers. The supraumbilical primary port is also frequently used in robotic surgery when increased inter port distances are desirable to eliminate robotic arm collisions. Reports in the literature describe the common locations of the supraumbilical port site are 5 cm above the umbilicus and at least 6 to 10 cm above a second-trimester gravid uterus or very large uterus and ovarian cyst. In an obese patient where umbilicus is displaced down, xiphisternum should be used to plan supraumbilical port. For upper abdominal surgery and most of the bariatric surgery, supraumbilical port incisions should be given 18cm below the xiphisternum.
Supra Umbilical Port
Infraumbilical Port
This port position is less commonly used in laparoscopic surgery. Infraumbilical port is used 3-5 cm below the umbilicus. Infraumbilical port should not be confused with the port of the inferior crease of umbilicus. This port position is used in the following surgery:
1. Single puncture sterilization
2. For upper abdominal surgery (Cholecystectomy or Duodenal Perforation) in very small height patients.
Primary Port Position
The central location and ability of the umbilicus to camouflage scars make it an attractive primary port site for laparoscopic surgery. There are many drawbacks to the umbilicus as well. The umbilicus is a naturally weak area due to the absence of all the layers. Weakness is also due to its location at the midpoint of the abdomen’s greatest diameter.
It is easy to believe that there is a difference between the umbilicus and other trocar sites in both susceptibilities to infection and postoperative incisional herniation.
The study showed that the increased infection rate at the umbilicus seems to be related to the retrieval of infected organs through the umbilicus and not to the umbilicus itself. When umbilicus was used to retrieve gallbladder after cholecystectomy the rate of infection was high due to port contamination with the infected gallbladder. Excluding cholecystectomy, the umbilical infection rate was two percent, similar to that of any alternative site. The postoperative ventral hernia rate was at 0.8 percent, the same at the umbilicus as elsewhere if the port more than 10 mm size is not repaired. It is now proved that the wound infection at the umbilicus is similar to that at other sites; postoperative ventral hernia at the umbilicus is similar to that at other sites and most of the infection after laparoscopic cholecystectomy is due to the contamination of wound due to infected gallbladder.
Secondary Port Position
The obligatory passage of the laparoscopic instruments through the abdominal wall generates a fixed point after which all movements are reversed. For instance, when the hand moves to the left, the end of the instrument moves right, and when the hand moves downwards, the end of the instrument moves upwards. For some surgeons, the fulcrum effect is not a problem, but for others, it is an insurmountable obstacle to the performance of advanced laparoscopy.
Because the handling of laparoscopic instruments is through the fixed point at the abdominal wall, the force feedback felt by the surgeon will depend on the length of the instrument inferior to this fixed point.
Baseball Diamond Concept of Port Position
A satisfactory relationship includes:
• An angle of 60° between the two instrument tips
• Tangential approach to the site
• Appropriate working distance
Baseball diamond concept of port position
First, decide the Target
Target may be in the suprapubic region for LAVH, right iliac fossa for appendicectomy, right upper quadrant for laparoscopic cholecystectomy, or left upper quadrant for fundoplication.
First, decide the target
Draw the Line of Optimum Area
For optimum task performance, half to the two-third instrument should be inside the abdomen. The size of the adult laparoscopic instrument is 36 cm and the pediatrics instrument is 28 cm.
Telescope and Instruments
• Telescope should be in the middle of the working instrument.
The telescope should be in the center of the working instrument
• Manipulation angle of instruments should be 60 degrees.
Manipulation angle 60° is the angle between tips of the instrument
Rule of Diamond for LAVH
These factors combined with the specific anatomy will determine individual port sites. For standard operations like cholecystectomy, standard port sites related to surface marking may suffice but as more advanced or varied situations are tackled we recommend that you master the skill of individual port placement using the internal view. In general, the optic and the two main operating ports usually lie at the points of a flattened triangle, the optic being centrally and more distally placed. Try to keep ports at least 5 cm apart.
Draw two arcs on the abdominal wall at 18 and 24 cm from that point and note area in between
Measure the length of the instrument
Manipulation angle 60° is essential for optimum task performance in laparoscopic surgery.
Drawbacks of Incorrect Port Position
Swording
Swording occurs when the telescope or the shaft of the assistant’s instrument obstructs the operator’s instruments. If this occurs you may need to consider:
• Repositioning retracting instruments
• Rotation of an angled telescope allowing alteration of the position of the end of the telescope
• Withdrawal of the telescope
• Transposition of the operator’s instruments
• Additional port placement
• Changing the instruments to a different port.
Port Positions
Port position for diagnostic laparoscopy
Port position for cholecystectomy
Alternative port position for cholecystectomy
Port position for appendectomy
Position for bilateral hernia, LAVH and most of the gynecological procedures





