Gasless Laparoscopic Surgery
Conventional laparoscopic surgery requires pneumoperitoneum to elevate the abdominal wall for proper exposure. A continuous insufflation of a non-combustible gas in a sealed environment is an essential part of minimal access surgery. Many undesirable physiological side effects have been observed with CO2 pneumoperitoneum. Furthermore, it has been necessary to retrain surgeons to use specialized instruments in order to operate on video images. Abdominal lifting mechanical devices can provide working space without pneumoperitoneum. With the gasless technique, conventional instruments can be used, direct visualization of abdominal viscera is possible, and digital examination of abdominal contents can be performed without the fear of loss exposure. Since these procedures are being performed in an isobaric abdominal cavity, the risk of body fluid contamination to the operating team is diminished when compared to open or traditional laparoscopic surgery. Gasless laparoscopic surgery is primarily advocated for the patients who are at high-risk of pneumoperitoneum. A variety of abdominal lift devices have been developed recently to provide good working space. Although gasless laparoscopic surgery is good for patients with a high risk of pneumoperitoneum, due to intraoperative problems and complications and because of suboptimal exposure, gasless laparoscopic surgery is still not considered as the prime modality for every patient. All the gasless systems can be used on their own or with low-pressure insufflation (4–6 mm Hg).
Three Basic Types
• Rubber tube sling abdominal wall lifts.
• Planar intraperitoneal abdominal wall retraction lift devices.
• Subcutaneous abdominal wall lift devices.
None of these techniques gives as good a laparoscopic exposure as the pressurized pneumoperitoneum because they produce a tent-like elevation of the abdominal wall rather than an elevated expansion and they do not depress the hollow organs and omentum. Exposure is improved when low-pressure insufflation is added.
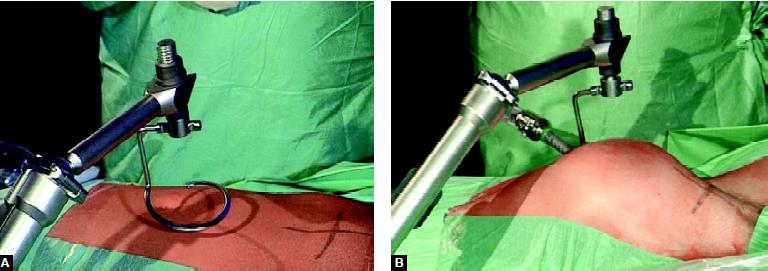
Several devices for gasless laparoscopy have been developed recently. The Laparolift (Origin Med systems) is a commercially available device routinely used by many surgeons and gynecologists worldwide. It consists of an adjustable arm that is attached to the side of the operating table and sterilely draped. The surgeon can raise and lower it electronically. The arm is connected to the Laparofan, a disposable sterile device with two metal blades (available in 10 and 15 cm lengths) that are inserted through the umbilical incision in an overlapped position. After entering the peritoneal space, the Laparofan paddles are spread. Using the dovetail connector, the Laparofan retractor is attached to the Laparolift arm and raised, creating a working cavity for laparoscopic surgery. It is intended to be used as a substitute for, or in conjunction with, pneumoperitoneum for abdominal wall retraction. The blades are then splayed out and locked into a V by tabs on the plastic handle, which is fixed to the end of the adjustable arm. The maximum lifting force of 13.6 kg is equivalent to a pneumoperitoneum pressure of 15 mm Hg. The laparoscope is inserted through the same incision, cephalad to the Laparofan.

Laparolift

Laparofan attached with Laparolift after introduction inside the abdominal cavity

Abdolift (another variety of abdominal lifting device)
The physiologic changes associated with CO 2 pneumoperitoneum are well tolerated in healthy patients but may result in life-threatening cardiac arrhythmia, myocardial infarction, cardiac failure, or pulmonary insufficiency in compromised patients who cannot compensate for these alterations is hemodynamic. A gasless laparoscopic approach could provide an added margin of safety for these patients. Patients undergoing laparoscopic surgery for malignancy or laparoscopically assisted vaginal hysterectomy may also benefit from gasless laparoscopy. Another potential advantage of gasless laparoscopy is the ability to use continuous suction and conventional laparotomy instruments.
Abdolift lifting the abdominal cavity

Use of open surgical instrument in gasless laparoscopic surgery
Disadvantages of Gasless Laparoscopic Surgery
• Marked guttering effect of lateral abdominal wall result after lifting the anterior abdominal wall.
• Anterior abdominal adhesion can make the insertion of this mechanical device difficult and visualization almost impossible.
• It is a space-occupying as an instrument takes all the ergonomically good space of port position.
• It only elevates anterior abdominal wall whereas gas creates workable space in the whole abdominal cavity.
• Sometime causes pressure necrosis of superior or inferior epigastric vessels.
• Bigger incision is required in the umbilicus.
• Difficult to perform in presence of ileus.
• Difficult peritoneal toileting at remote places.
Problems due to pneumoperitoneum
• Hypothermia
• Cardiac arrhythmia
• Cardiovascular collapse
• Pulmonary insufficiency
• Gas embolism
• Venous thrombosis
• Cerebral edema/ischemia
• Ocular hypertension
• Extraperitoneal insufflation (subcutaneous emphysema, pneumomediastinum)
Studies to date have demonstrated that surgical procedures with gasless laparoscopy are technically more difficult than those performed with adequate pneumoperitoneum owing to impaired visualization from the bowel in the pelvis. As with any new laparoscopic device, the initial enthusiasm over gasless laparoscopy has been tempered by actual clinical experience. However, because gasless laparoscopy still promises significant advantages over CO2 pneumoperitoneum in a high-risk patient, it is anticipated that interest in this technique will continue with improvements that will eliminate the current limitations to its use.
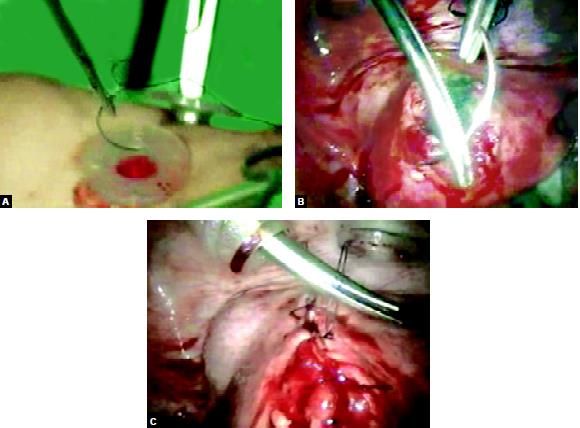 Use of open needle holder and suturing technique in gasless laparoscopy
Use of open needle holder and suturing technique in gasless laparoscopy
Open Vs closed Access Technique
Knowledge of proper access techniques is crucial to avoid these complications. However, no significant differences in overall complication rates have been found for closed compared with open techniques for primary abdominal insufflation, when performed by experienced surgeons. Proper selection of patients, knowledge of laparoscopic surgical anatomy, and attention to proper abdominal access techniques is necessary to avoid complications. Risk factors for complications include prior laparoscopy, abdominal adhesions, excessive bowel distention, very large abdominal or pelvic masses, and diaphragmatic hernia. Patients with a poor cardiopulmonary reserve may not tolerate pneumoperitoneum. For patients with risk factors for laparoscopic complications, open surgical access should be preferred.
Conventional laparoscopic surgery requires pneumoperitoneum to elevate the abdominal wall for proper exposure. A continuous insufflation of a non-combustible gas in a sealed environment is an essential part of minimal access surgery. Many undesirable physiological side effects have been observed with CO2 pneumoperitoneum. Furthermore, it has been necessary to retrain surgeons to use specialized instruments in order to operate on video images. Abdominal lifting mechanical devices can provide working space without pneumoperitoneum. With the gasless technique, conventional instruments can be used, direct visualization of abdominal viscera is possible, and digital examination of abdominal contents can be performed without the fear of loss exposure. Since these procedures are being performed in an isobaric abdominal cavity, the risk of body fluid contamination to the operating team is diminished when compared to open or traditional laparoscopic surgery. Gasless laparoscopic surgery is primarily advocated for the patients who are at high-risk of pneumoperitoneum. A variety of abdominal lift devices have been developed recently to provide good working space. Although gasless laparoscopic surgery is good for patients with a high risk of pneumoperitoneum, due to intraoperative problems and complications and because of suboptimal exposure, gasless laparoscopic surgery is still not considered as the prime modality for every patient. All the gasless systems can be used on their own or with low-pressure insufflation (4–6 mm Hg).
Three Basic Types
• Rubber tube sling abdominal wall lifts.
• Planar intraperitoneal abdominal wall retraction lift devices.
• Subcutaneous abdominal wall lift devices.
None of these techniques gives as good a laparoscopic exposure as the pressurized pneumoperitoneum because they produce a tent-like elevation of the abdominal wall rather than an elevated expansion and they do not depress the hollow organs and omentum. Exposure is improved when low-pressure insufflation is added.
Several devices for gasless laparoscopy have been developed recently. The Laparolift (Origin Med systems) is a commercially available device routinely used by many surgeons and gynecologists worldwide. It consists of an adjustable arm that is attached to the side of the operating table and sterilely draped. The surgeon can raise and lower it electronically. The arm is connected to the Laparofan, a disposable sterile device with two metal blades (available in 10 and 15 cm lengths) that are inserted through the umbilical incision in an overlapped position. After entering the peritoneal space, the Laparofan paddles are spread. Using the dovetail connector, the Laparofan retractor is attached to the Laparolift arm and raised, creating a working cavity for laparoscopic surgery. It is intended to be used as a substitute for, or in conjunction with, pneumoperitoneum for abdominal wall retraction. The blades are then splayed out and locked into a V by tabs on the plastic handle, which is fixed to the end of the adjustable arm. The maximum lifting force of 13.6 kg is equivalent to a pneumoperitoneum pressure of 15 mm Hg. The laparoscope is inserted through the same incision, cephalad to the Laparofan.
Laparolift
Laparofan attached with Laparolift after introduction inside the abdominal cavity
Abdolift (another variety of abdominal lifting device)
The physiologic changes associated with CO 2 pneumoperitoneum are well tolerated in healthy patients but may result in life-threatening cardiac arrhythmia, myocardial infarction, cardiac failure, or pulmonary insufficiency in compromised patients who cannot compensate for these alterations is hemodynamic. A gasless laparoscopic approach could provide an added margin of safety for these patients. Patients undergoing laparoscopic surgery for malignancy or laparoscopically assisted vaginal hysterectomy may also benefit from gasless laparoscopy. Another potential advantage of gasless laparoscopy is the ability to use continuous suction and conventional laparotomy instruments.
Abdolift lifting the abdominal cavity
Use of open surgical instrument in gasless laparoscopic surgery
Disadvantages of Gasless Laparoscopic Surgery
• Marked guttering effect of lateral abdominal wall result after lifting the anterior abdominal wall.
• Anterior abdominal adhesion can make the insertion of this mechanical device difficult and visualization almost impossible.
• It is a space-occupying as an instrument takes all the ergonomically good space of port position.
• It only elevates anterior abdominal wall whereas gas creates workable space in the whole abdominal cavity.
• Sometime causes pressure necrosis of superior or inferior epigastric vessels.
• Bigger incision is required in the umbilicus.
• Difficult to perform in presence of ileus.
• Difficult peritoneal toileting at remote places.
Problems due to pneumoperitoneum
• Hypothermia
• Cardiac arrhythmia
• Cardiovascular collapse
• Pulmonary insufficiency
• Gas embolism
• Venous thrombosis
• Cerebral edema/ischemia
• Ocular hypertension
• Extraperitoneal insufflation (subcutaneous emphysema, pneumomediastinum)
Studies to date have demonstrated that surgical procedures with gasless laparoscopy are technically more difficult than those performed with adequate pneumoperitoneum owing to impaired visualization from the bowel in the pelvis. As with any new laparoscopic device, the initial enthusiasm over gasless laparoscopy has been tempered by actual clinical experience. However, because gasless laparoscopy still promises significant advantages over CO2 pneumoperitoneum in a high-risk patient, it is anticipated that interest in this technique will continue with improvements that will eliminate the current limitations to its use.
Use of open needle holder and suturing technique in gasless laparoscopyOpen Vs closed Access Technique
Knowledge of proper access techniques is crucial to avoid these complications. However, no significant differences in overall complication rates have been found for closed compared with open techniques for primary abdominal insufflation, when performed by experienced surgeons. Proper selection of patients, knowledge of laparoscopic surgical anatomy, and attention to proper abdominal access techniques is necessary to avoid complications. Risk factors for complications include prior laparoscopy, abdominal adhesions, excessive bowel distention, very large abdominal or pelvic masses, and diaphragmatic hernia. Patients with a poor cardiopulmonary reserve may not tolerate pneumoperitoneum. For patients with risk factors for laparoscopic complications, open surgical access should be preferred.




