Laparoscopic Access in Cases of Morbid Obesity
In obese patients, the incision site should be transumbilical (base of the umbilicus) for the insertion of the Veress needle, because it is the thinnest abdominal wall and even in an obese patient, the amount of fat in trans umbilical region is less compared to other areas of the abdominal wall. The direction of the Veress needle entry in an obese patient should be perpendicular to the abdominal wall and the patient should be in a supine position not in Trendelenburg’s position. Once the Veress needle is inside pneumoperitoneum should be created up to 18 mm Hg. Once the actual pressure is equal to preset pressure and at least 1.5 to 3 liter of gas is introduced, the Veress needle is removed. After removing the Veress needle the initial incision is enlarged up to 11 mm. After enlarging the initial incision, fat should be cleared up to the anterior rectus sheath with the help of hemostat and little finger. In obese patients, it is difficult to lift the abdominal wall alone, the assistant’s hand should be asked for help to have a better grip. If bariatric surgery or fundoplication is planned, then the Veress needle and primary trocar need to be introduced supra umbilical so that the telescope can show the diaphragm and posterior mediastinum during esophageal mobilization.

The patient should be in a supine position not in Trendelenburg position
Abdominal access can be challenging in the patient with a thick abdominal wall; however, all types of entry access can be safely performed by experienced surgeons. In morbidly obese patients, the umbilicus is well below the aortic bifurcation in the supine position. When using the Veress needle technique in obese patients, the left upper quadrant is preferred by many surgeons for initial placement (Palmer's point). If supraumbilical access is used to perform a bariatric surgery assistant’s help should be taken to lift the abdominal wall. Longer ports 20cm in length are required in the case of the obese patient.

Veress needle introduction in an obese patient
The irrigation test, aspiration test, the saline drop test, and an opening pressure of less than 10 mmHg should all be used to confirm the proper placement of the needle. When using the Hassan technique for patients with a large amount of subcutaneous fat, the incision should be made large enough to identify the abdominal wall fascia and peritoneum. The area beneath the Veress needle insertion site inside the abdomen should be inspected for injuries during the initial laparoscopic evaluation of the abdomen.

Optical trocar entry in obese patients
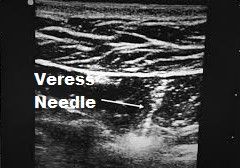
Ultrasound Visceral Slide
There is a simple preoperative test that can help to identify a safe region for Veress needle insertion in the scarred abdomen. The preoperative detection of anterior abdominal wall adhesions by ultrasonic scanning is a simple and reliable technique of ultrasonic detection and mapping of abdominal wall adhesions. In patients with portal hypertension, a major risk factor upon entry into the abdomen is an injury to large, engorged paraumbilical vessels in the anterior abdominal wall. Major blood loss often results from just entering the abdomen. The use of ultrasound-guided access into the peritoneum for laparoscopic surgery is also a safe and effective approach in a patient presenting with portal hypertension. This technique demonstrates an effective tool in the surgical armamentarium for entering the abdomen in patients with caput-medusae. Once the Veress needle has been inserted, there should still be concern about the risk of causing damage to the trocar. The following techniques have been described for this situation.
Ultrasound-guided entry
Sounding Test
A fine spinal needle, attached to a saline-filled syringe, is passed into the inflated abdomen. As the needle is slowly advanced, while aspirating, a stream of bubbles is seen in the saline until the needle tip contacts tissue. The needle is then withdrawn towards the surface and the process repeated several times, in different directions, thereby “mapping” the gas-filled cavity and any solid structures.
In obese patients, the incision site should be transumbilical (base of the umbilicus) for the insertion of the Veress needle, because it is the thinnest abdominal wall and even in an obese patient, the amount of fat in trans umbilical region is less compared to other areas of the abdominal wall. The direction of the Veress needle entry in an obese patient should be perpendicular to the abdominal wall and the patient should be in a supine position not in Trendelenburg’s position. Once the Veress needle is inside pneumoperitoneum should be created up to 18 mm Hg. Once the actual pressure is equal to preset pressure and at least 1.5 to 3 liter of gas is introduced, the Veress needle is removed. After removing the Veress needle the initial incision is enlarged up to 11 mm. After enlarging the initial incision, fat should be cleared up to the anterior rectus sheath with the help of hemostat and little finger. In obese patients, it is difficult to lift the abdominal wall alone, the assistant’s hand should be asked for help to have a better grip. If bariatric surgery or fundoplication is planned, then the Veress needle and primary trocar need to be introduced supra umbilical so that the telescope can show the diaphragm and posterior mediastinum during esophageal mobilization.
The patient should be in a supine position not in Trendelenburg position
Abdominal access can be challenging in the patient with a thick abdominal wall; however, all types of entry access can be safely performed by experienced surgeons. In morbidly obese patients, the umbilicus is well below the aortic bifurcation in the supine position. When using the Veress needle technique in obese patients, the left upper quadrant is preferred by many surgeons for initial placement (Palmer's point). If supraumbilical access is used to perform a bariatric surgery assistant’s help should be taken to lift the abdominal wall. Longer ports 20cm in length are required in the case of the obese patient.
Veress needle introduction in an obese patient
The irrigation test, aspiration test, the saline drop test, and an opening pressure of less than 10 mmHg should all be used to confirm the proper placement of the needle. When using the Hassan technique for patients with a large amount of subcutaneous fat, the incision should be made large enough to identify the abdominal wall fascia and peritoneum. The area beneath the Veress needle insertion site inside the abdomen should be inspected for injuries during the initial laparoscopic evaluation of the abdomen.
Optical trocar entry in obese patients
Ultrasound Visceral Slide
There is a simple preoperative test that can help to identify a safe region for Veress needle insertion in the scarred abdomen. The preoperative detection of anterior abdominal wall adhesions by ultrasonic scanning is a simple and reliable technique of ultrasonic detection and mapping of abdominal wall adhesions. In patients with portal hypertension, a major risk factor upon entry into the abdomen is an injury to large, engorged paraumbilical vessels in the anterior abdominal wall. Major blood loss often results from just entering the abdomen. The use of ultrasound-guided access into the peritoneum for laparoscopic surgery is also a safe and effective approach in a patient presenting with portal hypertension. This technique demonstrates an effective tool in the surgical armamentarium for entering the abdomen in patients with caput-medusae. Once the Veress needle has been inserted, there should still be concern about the risk of causing damage to the trocar. The following techniques have been described for this situation.
Ultrasound-guided entry
Sounding Test
A fine spinal needle, attached to a saline-filled syringe, is passed into the inflated abdomen. As the needle is slowly advanced, while aspirating, a stream of bubbles is seen in the saline until the needle tip contacts tissue. The needle is then withdrawn towards the surface and the process repeated several times, in different directions, thereby “mapping” the gas-filled cavity and any solid structures.




