Transobturator Tape
When tension-free vaginal tape (TVT) was first introduced into clinical practice in the mid-to-late 1990s, the gold standard surgical procedure in the treatment of stress urinary incontinence was the Burch colposuspension. Several randomized controlled trials have compared the efficacy and safety of these two procedures and shown that TVT has a lower morbidity rate and equal or superior efficacy at midterm follow-up. TVT has gradually replaced the colposuspension as the first choice procedure, especially now that the long-term results (5–7-year outcome) are known (81.3% and 82% cure rate).
There are, however, concerns over the safety of TVT. A Finnish series of 1455 women treated for stress urinary incontinence demonstrated several vascular injuries (venous lacerations were the most frequent injury reported), while Zilbert et al reported a case of right external iliac artery injury. In addition, two deaths due to serious vascular injuries have been reported to the manufacturers, as have bowel perforations. Most of these complications are related to the penetration of the retropubic space. In order to avoid these complications, but keep the principle of a minimally invasive procedure to reinforce the structures supporting the urethra, Delorme described the transobturator tape (TOT). In this technique, a 2 cm incision is made through the vagina over the urethra, and a tunnel created out to the obturator foramen on either side. A trocar is then passed from the thigh fold through the obturator foramen from the outside to the inside and brought round through the vaginal incision. A multifilament microporous tape is then fed through the trocar and brought through the obturator foramen. The procedure is repeated on both sides and the tape left under no tension under the mid urethra. De Leval et al described a further modification to the surgical technique, which allows the passage of a trocar and tape through the obturator foramen from inside to out. The authors felt that this further reduced any risk of damage to the urethra and bladder; however, the long-term safety of this type of procedure is not known.

Removal of plastic tape with cutting the excessive mesh

Scissors or forceps should be placed between the urethra and the tape
The tension-free vaginal tape has revolutionized the surgical treatment of stress urinary incontinence but remains an abdominal procedure with all of the potential complications therein. The transobturator tape procedure described here produces the same end result, i.e. a tension-free tape left under the mid urethra, but without the risks of an abdominal procedure. Bladder perforation is the most common complication occurring during the TVT procedure, with the incidence reported as between 0.8 percent and 21 percent. However, with the TOT procedure, the risk of bladder perforation is significantly reduced.
Injuries in TVT procedure

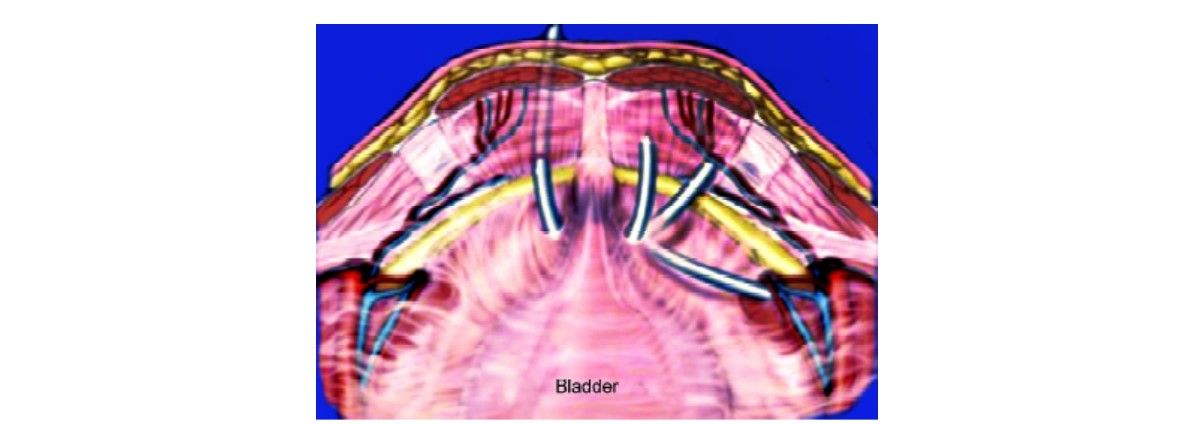
Pelvic anatomy demonstrating obturator foramen
Functional Theories and Comparison with Tension-free Vaginal Tape
DeLancey's theories on pelvic support for the bladder and urethra help to explain the mechanism of action of the transobturator tape in the treatment of stress urinary incontinence, in that the position of the tape is similar to that of the natural hammock supporting the urethra. The TOT procedure using polypropylene tape satisfies most of the requirements for effective surgery. In the medium-term the results are satisfactory and, unlike the retropubic tape (TVT), the purely perineal location of the transobturator tape minimizes the risk of trauma to the bladder, intestine, major vessels and nerves.
When tension-free vaginal tape (TVT) was first introduced into clinical practice in the mid-to-late 1990s, the gold standard surgical procedure in the treatment of stress urinary incontinence was the Burch colposuspension. Several randomized controlled trials have compared the efficacy and safety of these two procedures and shown that TVT has a lower morbidity rate and equal or superior efficacy at midterm follow-up. TVT has gradually replaced the colposuspension as the first choice procedure, especially now that the long-term results (5–7-year outcome) are known (81.3% and 82% cure rate).
There are, however, concerns over the safety of TVT. A Finnish series of 1455 women treated for stress urinary incontinence demonstrated several vascular injuries (venous lacerations were the most frequent injury reported), while Zilbert et al reported a case of right external iliac artery injury. In addition, two deaths due to serious vascular injuries have been reported to the manufacturers, as have bowel perforations. Most of these complications are related to the penetration of the retropubic space. In order to avoid these complications, but keep the principle of a minimally invasive procedure to reinforce the structures supporting the urethra, Delorme described the transobturator tape (TOT). In this technique, a 2 cm incision is made through the vagina over the urethra, and a tunnel created out to the obturator foramen on either side. A trocar is then passed from the thigh fold through the obturator foramen from the outside to the inside and brought round through the vaginal incision. A multifilament microporous tape is then fed through the trocar and brought through the obturator foramen. The procedure is repeated on both sides and the tape left under no tension under the mid urethra. De Leval et al described a further modification to the surgical technique, which allows the passage of a trocar and tape through the obturator foramen from inside to out. The authors felt that this further reduced any risk of damage to the urethra and bladder; however, the long-term safety of this type of procedure is not known.
Removal of plastic tape with cutting the excessive mesh
Scissors or forceps should be placed between the urethra and the tape
The tension-free vaginal tape has revolutionized the surgical treatment of stress urinary incontinence but remains an abdominal procedure with all of the potential complications therein. The transobturator tape procedure described here produces the same end result, i.e. a tension-free tape left under the mid urethra, but without the risks of an abdominal procedure. Bladder perforation is the most common complication occurring during the TVT procedure, with the incidence reported as between 0.8 percent and 21 percent. However, with the TOT procedure, the risk of bladder perforation is significantly reduced.
Injuries in TVT procedure
Pelvic anatomy demonstrating obturator foramen
Functional Theories and Comparison with Tension-free Vaginal Tape
DeLancey's theories on pelvic support for the bladder and urethra help to explain the mechanism of action of the transobturator tape in the treatment of stress urinary incontinence, in that the position of the tape is similar to that of the natural hammock supporting the urethra. The TOT procedure using polypropylene tape satisfies most of the requirements for effective surgery. In the medium-term the results are satisfactory and, unlike the retropubic tape (TVT), the purely perineal location of the transobturator tape minimizes the risk of trauma to the bladder, intestine, major vessels and nerves.





