Tension-free Vaginal Tape
Stress urinary incontinence or genuine stress incontinence is a problem of the urinary bladder where the urethral sphincter weakens and as a result, cannot prevent the flow of urine through it when the intra-abdominal pressure rises such as in coughing, sneezing, lifting something heavy or even standing or walking.
There are several causes of urethral sphincter weakness, most common being:
• Unattended pregnancy and childbirth
• Frequent heavy lifting
• Estrogen deficiency or menopause
• Obesity.
Urinary incontinence is reported by 14 percent of women, and urodynamic stress incontinence, the involuntary leakage of urine during increased abdominal pressure in the absence of a detrusor contraction is diagnosed in over half of the women presenting to hospital with urinary incontinence. Systematic reviews have shown that colposuspension has the best surgical results when compared with other treatments for urodynamic stress incontinence, with cure rates of up to 90 percent in women who have had no previous surgery for incontinence, although there are only limited data from randomized trials on which to base clinical practice. Although colposuspension remains the most popular choice for the treatment of stress incontinence, some authors have reported less than half of patients remaining dry and free of complications long-term. Complications include hemorrhage, hematoma, bladder injury, and urinary tract infection. Up to 20 percent of women may develop de novo detrusor overactivity; voiding dysfunction has been reported in 3 percent to 32 percent of women, and surgery for vaginal prolapse may be required in 2.5 percent to 26.7 percent after the procedure.
Minimally invasive suburethral sling procedures have become a mainstay for the surgical treatment of stress urinary incontinence in women. The transvaginal tape is a minimally invasive procedure for women who suffer from stress urinary incontinence. In the transvaginal tape, the urinary bladder and urethra are repaired, strengthened, and returned to its original position in the pelvis. Tension-free vaginal tape (also known as TVT) was first introduced in Sweden in the mid-1990s by Ulf Ulmsten and Papa Petros. The American Urological Association (AUA) has established a task force to determine the most effective operations for the treatment of stress urinary incontinence. They concluded the most curative operations as published in the worldwide medically indexed literature: Burch urethral suspension procedure and the suburethral sling operation. Cure rates for both procedures were found to fall routinely between 80 to 90 percent. The TVT operation is a “sling” operation and its cure rate falls within the international standards of a cure for other types of sling procedures. The tension-free vaginal tape procedure is a relatively recent treatment for stress incontinence.
Polypropylene tape is inserted suburethral under local anesthesia with sedation. The procedure is thought to work by providing a pubourethral “neoligament”. Increased intraabdominal pressure results in a kink at the point of fixation, which prevents urine flow.
Tension-free Vaginal Tape
Surgical Technique
The patient should be placed in the lithotomy position taking care to avoid hip flexion greater than 60°. The procedure can be carried out under local anesthesia, but it can also be performed using regional or general anesthesia. The extent of dissection is minimal, i.e. a vaginal midline entry with a small paraurethral dissection to initially position the needle and two suprapubic skin incisions. Using forceps, grasp the vaginal wall at each side of the urethra. Using a small scalpel, make a sagittal incision about 1.5 cm long starting approximately 1.0 cm from the outer urethral meatus. This incision will cover the mid-urethral zone and will allow for the subsequent passage of the sling (tape).
With a small pair of blunt scissors, two small paraurethral dissections (approximately 0.5 cm) are made so that the tip of the needle can then be introduced into or passed through the paraurethral dissection. Then, two abdominal skin incisions of 0.5 to 1 cm are made one on each side of the midline just above the symphysis not more than 4 to 5 cm apart. Incision placement and needle passage near the midline and close to the back of the pubic bone are important to avoid anatomic structures in the inguinal area and lateral pelvic sidewall. The TVT rigid catheter guide is inserted into the channel of the Foley catheter (18 French). The handle of the guide is fixed around the catheter, proximal to its widening. The purpose of the guide is to move the bladder neck and urethra away from where the tip of the needle will pass into the retropubic space.
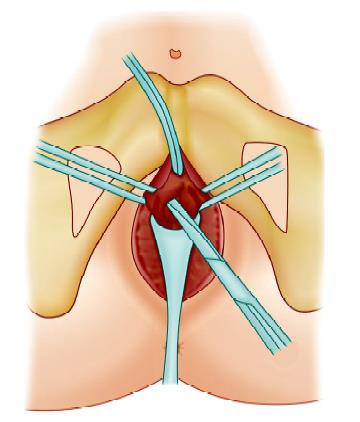
The abdominal and vaginal incision for tension-free vaginal type (TVT)
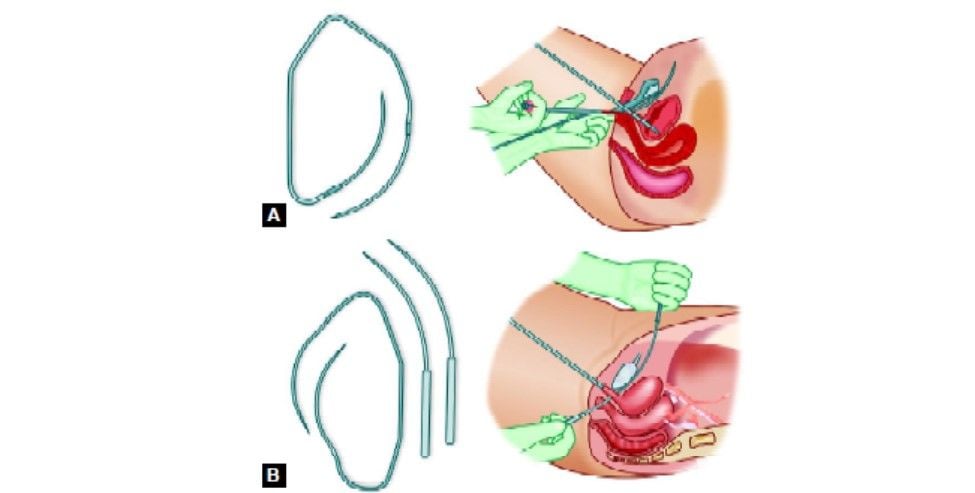
Passage of needle through retropubic space
Via use of the Foley catheter and the rigid catheter guide, the urethra and bladder are moved contralaterally to the side of the needle passage. During this maneuver, the bladder should be empty. Using the introducer, the needle is passed paraurethral penetrating the urogenital diaphragm. Insertion and passage are controlled by using the long or index finger in the vagina under the vaginal wall on the ipsilateral side and fingertip control on the pelvic rim. The curved part of the needle should rest in the palm of the “vaginal” hand.
If you are right-handed this means that the left hand generally is the one to be used for needle guidance. On the other hand, grip the handle of the introducer gently. Now introduce the needle tip into the retropubic space. Once again, observe that this should be done by the palm of the vaginal hand and with the needle tip horizontally, i.e. in the frontal plane. After the passage of the urogenital diaphragm, you will feel that the resistance is significantly reduced. Immediately aim the tip of the needle towards the abdominal midline and lower the handle of the introducer thereby pressing the tip of the needle against the back of the pubic bone. Now, move the needle tip upwards to the abdominal skin incision, keeping in close contact with the pubic bone all the way. When the needle tip has reached the abdominal incision, cystoscopy is performed to confirm bladder integrity. The bladder must be emptied after the first cystoscopy. Disarticulate the reusable introducer and pull the remaining portion of the TVT needle through the abdominal incision. The procedure is then repeated on the other side.
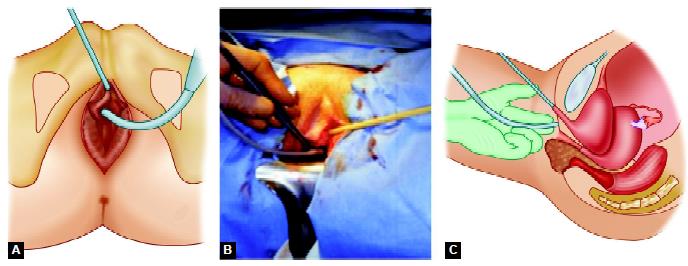
The safe entry of needle with the use of a urethral catheter guide
The needles are then pulled upward to bring the tape (sling) loosely, i.e. without tension, under the mid urethra. Cut the tape close to the needles. Now, adjust the tape so that leakage is reduced allowing a few drops of urinary leakage to occur under stress. For this, use patient feedback, i.e. coughing with a full bladder (approximately 300 ml) and keep the vaginal incision temporarily closed by a gentle grip with small forceps. The plastic sheaths that surround the tape are then removed. To avoid putting tension on the tape, a blunt instrument (scissors or forceps) should be placed between the urethra and the tape during removal of the plastic sheaths. Premature removal of the sheath may make subsequent adjustments difficult. After proper adjustment of the tape, close the vaginal incision. The abdominal ends of the tape are then cut and left in subcutis. Do not suture them. Suture the skin incisions. Empty the bladder. Following this procedure, postoperative catheterization is not typically required. The patient should be encouraged to try to empty the bladder 2 to 3 hours after the operation.
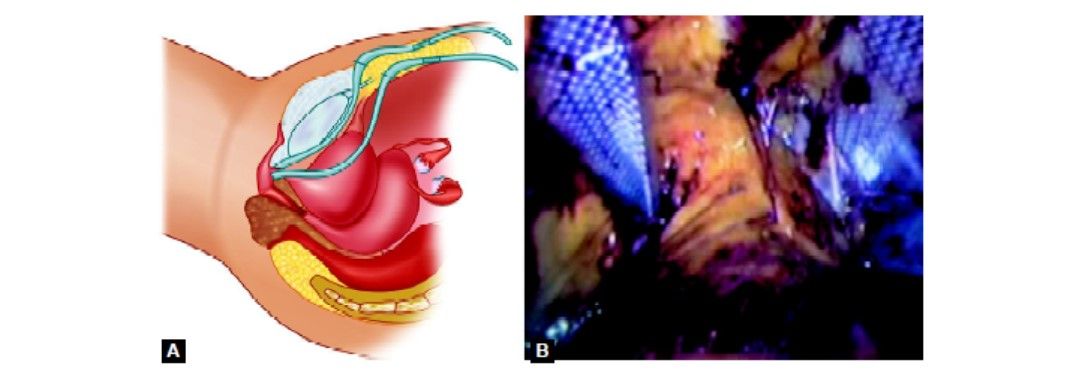
Completed application of tape with a laparoscopic view
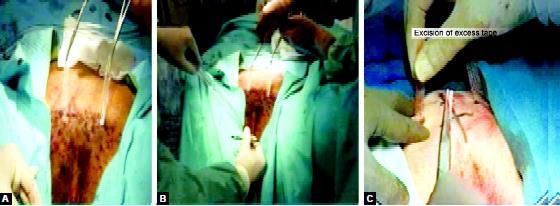
Removal of plastic tape with cutting the excessive mesh
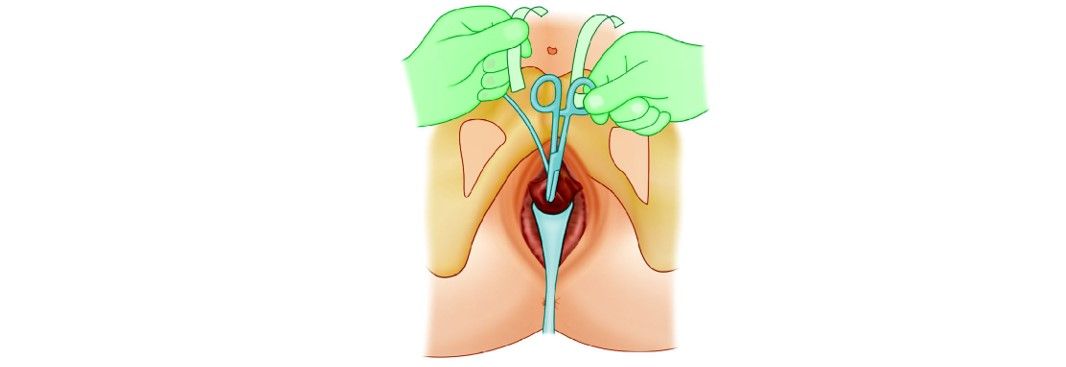
Scissors or forceps should be placed between the urethra and the tape
Stress urinary incontinence or genuine stress incontinence is a problem of the urinary bladder where the urethral sphincter weakens and as a result, cannot prevent the flow of urine through it when the intra-abdominal pressure rises such as in coughing, sneezing, lifting something heavy or even standing or walking.
There are several causes of urethral sphincter weakness, most common being:
• Unattended pregnancy and childbirth
• Frequent heavy lifting
• Estrogen deficiency or menopause
• Obesity.
Urinary incontinence is reported by 14 percent of women, and urodynamic stress incontinence, the involuntary leakage of urine during increased abdominal pressure in the absence of a detrusor contraction is diagnosed in over half of the women presenting to hospital with urinary incontinence. Systematic reviews have shown that colposuspension has the best surgical results when compared with other treatments for urodynamic stress incontinence, with cure rates of up to 90 percent in women who have had no previous surgery for incontinence, although there are only limited data from randomized trials on which to base clinical practice. Although colposuspension remains the most popular choice for the treatment of stress incontinence, some authors have reported less than half of patients remaining dry and free of complications long-term. Complications include hemorrhage, hematoma, bladder injury, and urinary tract infection. Up to 20 percent of women may develop de novo detrusor overactivity; voiding dysfunction has been reported in 3 percent to 32 percent of women, and surgery for vaginal prolapse may be required in 2.5 percent to 26.7 percent after the procedure.
Minimally invasive suburethral sling procedures have become a mainstay for the surgical treatment of stress urinary incontinence in women. The transvaginal tape is a minimally invasive procedure for women who suffer from stress urinary incontinence. In the transvaginal tape, the urinary bladder and urethra are repaired, strengthened, and returned to its original position in the pelvis. Tension-free vaginal tape (also known as TVT) was first introduced in Sweden in the mid-1990s by Ulf Ulmsten and Papa Petros. The American Urological Association (AUA) has established a task force to determine the most effective operations for the treatment of stress urinary incontinence. They concluded the most curative operations as published in the worldwide medically indexed literature: Burch urethral suspension procedure and the suburethral sling operation. Cure rates for both procedures were found to fall routinely between 80 to 90 percent. The TVT operation is a “sling” operation and its cure rate falls within the international standards of a cure for other types of sling procedures. The tension-free vaginal tape procedure is a relatively recent treatment for stress incontinence.
Polypropylene tape is inserted suburethral under local anesthesia with sedation. The procedure is thought to work by providing a pubourethral “neoligament”. Increased intraabdominal pressure results in a kink at the point of fixation, which prevents urine flow.
Tension-free Vaginal Tape
Surgical Technique
The patient should be placed in the lithotomy position taking care to avoid hip flexion greater than 60°. The procedure can be carried out under local anesthesia, but it can also be performed using regional or general anesthesia. The extent of dissection is minimal, i.e. a vaginal midline entry with a small paraurethral dissection to initially position the needle and two suprapubic skin incisions. Using forceps, grasp the vaginal wall at each side of the urethra. Using a small scalpel, make a sagittal incision about 1.5 cm long starting approximately 1.0 cm from the outer urethral meatus. This incision will cover the mid-urethral zone and will allow for the subsequent passage of the sling (tape).
With a small pair of blunt scissors, two small paraurethral dissections (approximately 0.5 cm) are made so that the tip of the needle can then be introduced into or passed through the paraurethral dissection. Then, two abdominal skin incisions of 0.5 to 1 cm are made one on each side of the midline just above the symphysis not more than 4 to 5 cm apart. Incision placement and needle passage near the midline and close to the back of the pubic bone are important to avoid anatomic structures in the inguinal area and lateral pelvic sidewall. The TVT rigid catheter guide is inserted into the channel of the Foley catheter (18 French). The handle of the guide is fixed around the catheter, proximal to its widening. The purpose of the guide is to move the bladder neck and urethra away from where the tip of the needle will pass into the retropubic space.
The abdominal and vaginal incision for tension-free vaginal type (TVT)
Passage of needle through retropubic space
Via use of the Foley catheter and the rigid catheter guide, the urethra and bladder are moved contralaterally to the side of the needle passage. During this maneuver, the bladder should be empty. Using the introducer, the needle is passed paraurethral penetrating the urogenital diaphragm. Insertion and passage are controlled by using the long or index finger in the vagina under the vaginal wall on the ipsilateral side and fingertip control on the pelvic rim. The curved part of the needle should rest in the palm of the “vaginal” hand.
If you are right-handed this means that the left hand generally is the one to be used for needle guidance. On the other hand, grip the handle of the introducer gently. Now introduce the needle tip into the retropubic space. Once again, observe that this should be done by the palm of the vaginal hand and with the needle tip horizontally, i.e. in the frontal plane. After the passage of the urogenital diaphragm, you will feel that the resistance is significantly reduced. Immediately aim the tip of the needle towards the abdominal midline and lower the handle of the introducer thereby pressing the tip of the needle against the back of the pubic bone. Now, move the needle tip upwards to the abdominal skin incision, keeping in close contact with the pubic bone all the way. When the needle tip has reached the abdominal incision, cystoscopy is performed to confirm bladder integrity. The bladder must be emptied after the first cystoscopy. Disarticulate the reusable introducer and pull the remaining portion of the TVT needle through the abdominal incision. The procedure is then repeated on the other side.
The safe entry of needle with the use of a urethral catheter guide
The needles are then pulled upward to bring the tape (sling) loosely, i.e. without tension, under the mid urethra. Cut the tape close to the needles. Now, adjust the tape so that leakage is reduced allowing a few drops of urinary leakage to occur under stress. For this, use patient feedback, i.e. coughing with a full bladder (approximately 300 ml) and keep the vaginal incision temporarily closed by a gentle grip with small forceps. The plastic sheaths that surround the tape are then removed. To avoid putting tension on the tape, a blunt instrument (scissors or forceps) should be placed between the urethra and the tape during removal of the plastic sheaths. Premature removal of the sheath may make subsequent adjustments difficult. After proper adjustment of the tape, close the vaginal incision. The abdominal ends of the tape are then cut and left in subcutis. Do not suture them. Suture the skin incisions. Empty the bladder. Following this procedure, postoperative catheterization is not typically required. The patient should be encouraged to try to empty the bladder 2 to 3 hours after the operation.
Completed application of tape with a laparoscopic view
Removal of plastic tape with cutting the excessive mesh
Scissors or forceps should be placed between the urethra and the tape




