Laparoscopic Tissue Retrieval Technique
One of the limitations of minimal access surgery is difficulty in the retrieval of tissue. Previously surgeons were reluctant to perform many of the advanced surgical procedures due to this difficult procedure. New techniques for removing tissue have helped increase the number and types of laparoscopic surgeries that can be done laparoscopically. Safe removal of tissue is an important consideration in laparoscopic surgery and applies to all specimens irrespective of whether they are thought to be benign or malignant. The importance of wound protection is shown by considering laparoscopic cholecystectomy for symptomatic gallstone disease. Most of the gallbladders at the time of retrieval can be squeezed out through an unprotected port wound. At the time of extraction, the exit wound must be of sufficient size, and wound protection should be used to ensure that there is no contact between the specimen and the abdominal wall during removal. We all know that the incidence of unsuspected gallbladder cancer is between 0.5 and 1 percent and there are reported cases of port site tumor nodules because of implantation of tumor cells after extraction of the gallbladder through an unprotected wound.
Tissue reduction enables extraction through small wounds but can be used only for benign specimens. Tissue reduction can be carried out by various techniques, including mechanical fragmentation and morcellation. It should be done inside a rip-proof bag whenever possible. This is essential for laparoscopic splenectomy to prevent implantation of splenic fragments on the serosal surfaces, which leads to selenosis. Most commonly the resected tissue should be hidden under the port and then everything should come together with the port. This technique is used for most of the small size organs like the appendix, gallbladder, small ovarian cyst, ectopic pregnancy, salpingectomy, small oophorectomy, etc.
Endobags
In some cases, the tissue to be removed is first encased in a specimen retrieval bag. These tissue retrieval bags are available in the market and can be prepared by the surgeon himself at the time of laparoscopic surgery. For infected tissue and in case of suspected carcinoma, tissue retrieval bag should be used. Many sizes of disposable tissue retrieval bags are available and hard rim of these retrieval bags is easy to negotiate inside the abdominal cavity. One can easily make the retrieval bag by tying and cutting the fingers of sterilized gloves. If the gloves used for the retrieval of tissue, it should be used carefully. It should not puncture while removing from the abdominal cavity.
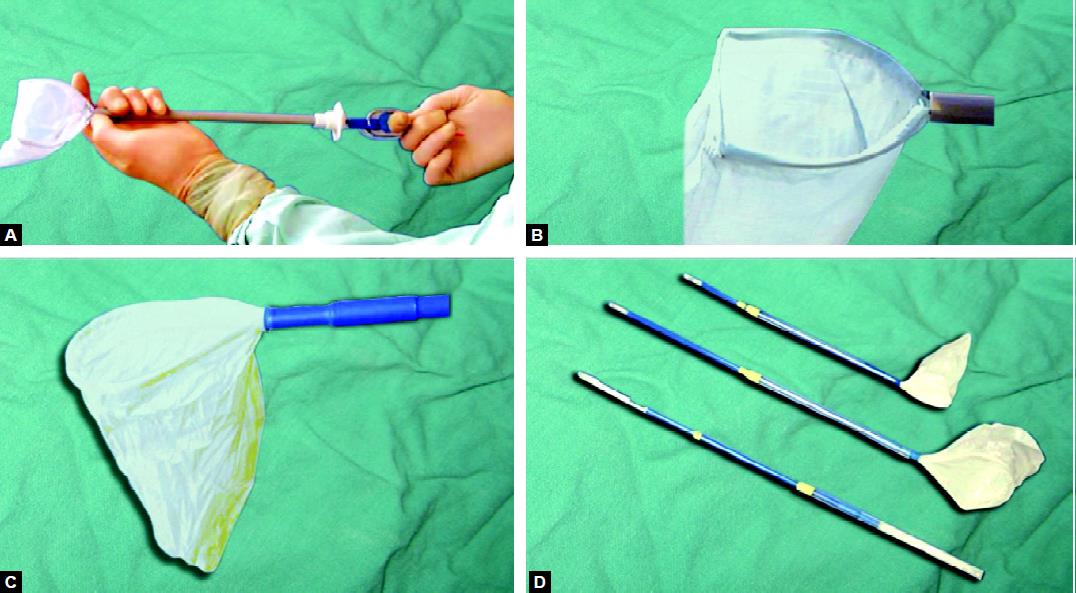
Disposable endobags

Endobags
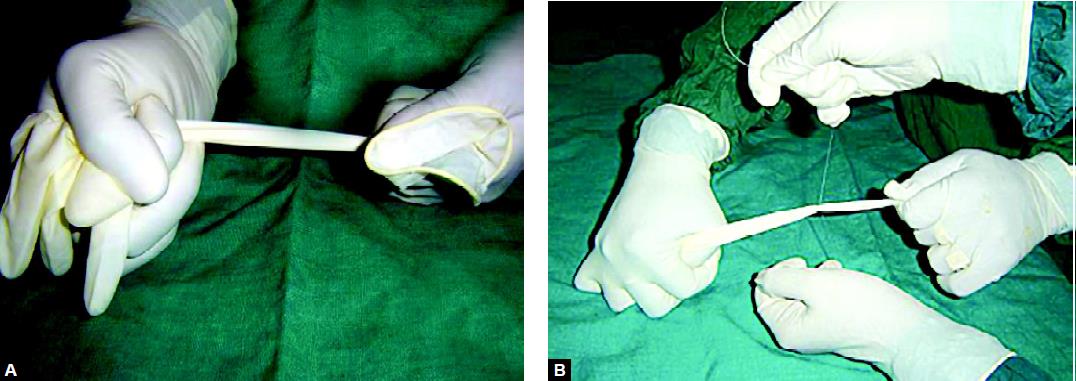
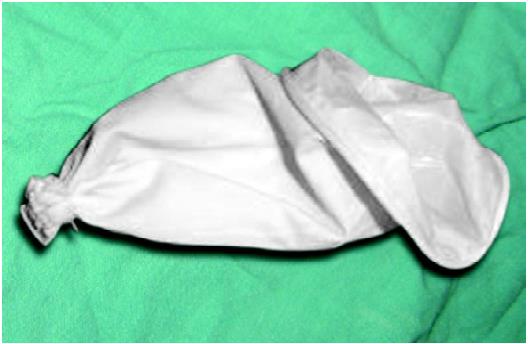
The glove is kept stretched while one assistant will tie it in the middle. Keeping it stretched will create a good dumbbell after knotting and so there is no chance of slipping of knot inside the abdominal cavity. The latex material used to manufacture gloves sometimes, react with human tissue and it can create a problem if the glove is punctured and a piece of latex is left inside the human body. Most commonly this torn piece of gloves can be missed in the layers of the abdominal wall. At the time of the introduction of glove endobag, it should be held by its cut end and kept stretched over the shaft of grasper to decrease its thickness. The polythene covering of ryels tube can also be used as an inexpensive readymade retrieval bag. This is sterilized and open at one end. These polythene bags can be used as an excellent retrieval pouch if used carefully. The polythene bags have one demerit that sometimes the edges are difficult to find out because it is transparent and secondly because it is thin and does not have an elastic property like gloves so it slips easily after once held by the grasper. The drawback of this self-made retrieval bag is that they do not have hard ream so it is difficult to manipulate inside the abdominal cavity. These bags can be introduced inside the abdominal cavity through 10 mm ports. In special circumstances, if there is difficulty is found it can be introduced directly through the port wound after withdrawing the cannula. Once the retrieval bag is inside it should be positioned in free abdominal space and the rim of the bag should be stabilized with nondominant hand and the dominant hand should be used to put the specimen inside. Once the bag is inside the abdominal cavity both the edges of the retrieval bag should be lifted to displace the specimen into the base of the bag. Condom can also be used for retrieving tissue. The lubricated condom should be avoided because it can cause tissue reaction. To take the specimen out, the surgeon should hide the mouth of the retrieval bag inside the cannula by pulling it and then the cannula together with the neck of the bag is pulled outside the abdominal cavity.
Once the neck of the bag is out, its opening is stretched with the help of an assistant. Ovum forceps can be introduced inside to morcellate the tissue manually if there is difficulty in pulling the bag out.
Making endobag with a glove
Glove endobag

Way of introducing endobag

Using glove endobag
Colpotomy
For large size gynecological tissue, the colpotomy route is good for retrieval. Colpotomy can be done laparoscopically with the help of a heal of the hook. Counter pushing by other instruments is effective. Sponge over sponge holding forceps is inserted in posterior vaginal fornix by one assistant and the surgeon cuts the vaginal fascia between both the uterosacral ligaments with the heel of the hook.
Hand-Assisted Laparoscopic Surgery
The hand-assisted technique was initially started keeping inside the ease of tissue retrievals, wherein the surgeon uses his or her hand, inserted through the initial incision, to aid in the exploration, isolation, and removal of tissue. The hand-assisted technique offers distinct advantages, the superior visualization afforded by the laparoscope, and a tactile component that is important in many aspects of surgery and has allowed surgeons to apply a less invasive approach to surgeries that previously could not have been done laparoscopically. Hand-assisted laparoscopy can also serve as a bridge between open surgery and straight laparoscopy, making it easier for surgeons to practice and learn the skills necessary for performing laparoscopic procedures.
Morcellator
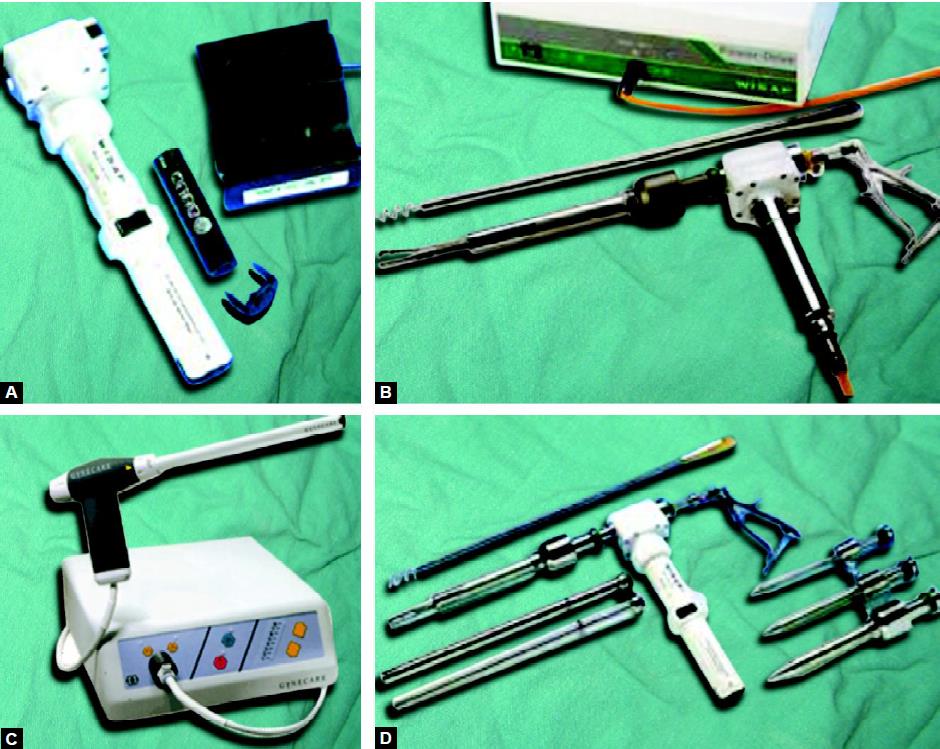
The use of a morcellator is another way that facilitates the grinding of solid tissue and then these can be taken out without any difficulty. Recently many companies have launched a battery-operated morcellator. The morcellator is an important instrument for tissue retrieval in myomectomy and splenectomy. One of the early concerns about laparoscopic procedures in cancer patients was that they caused port site metastases, i.e. the appearance of recurrent tumor tissue at the site of trocar entry.

Electrical morcellator
Different type of morcellator
Morcellation of tissue
Cancer surgery, however, poses some unique challenges that make the application of laparoscopic surgery in oncology more problematic. It is critically important in cancer that whole organs should be removed intact (en bloc) so that pathologists can properly examine them and measure and document the depths and margins of tumor invasion. A second concern for surgical oncologists is cell transfer or cell spillage. Diseased tissue must be removed without contaminating adjacent tissues and structures with cancer cells. Because of these concerns, tissue morcellation, a technique commonly used in noncancer laparoscopic surgery in which the tissue is divided into pieces so that it can be removed more easily should not be used for oncologic procedures. All the 10 mm or greater than 10 mm defects should be closed properly to prevent any future possibility of a hernia. The suture passer should be used to pass the thread and then it should be tied externally. Especially, designed port closure instruments are also available commercially. If the port is suddenly taken out, the chances of port site hernia and adhesion are much higher. It is a good practice to insert some blunt instrument while removing the last port out, to prevent entrapment of omentum or bowel content. After closing the rectus sheath the skin can be closed by intradermal, skin stapler, or by any of the surgical skin glues available.
One of the limitations of minimal access surgery is difficulty in the retrieval of tissue. Previously surgeons were reluctant to perform many of the advanced surgical procedures due to this difficult procedure. New techniques for removing tissue have helped increase the number and types of laparoscopic surgeries that can be done laparoscopically. Safe removal of tissue is an important consideration in laparoscopic surgery and applies to all specimens irrespective of whether they are thought to be benign or malignant. The importance of wound protection is shown by considering laparoscopic cholecystectomy for symptomatic gallstone disease. Most of the gallbladders at the time of retrieval can be squeezed out through an unprotected port wound. At the time of extraction, the exit wound must be of sufficient size, and wound protection should be used to ensure that there is no contact between the specimen and the abdominal wall during removal. We all know that the incidence of unsuspected gallbladder cancer is between 0.5 and 1 percent and there are reported cases of port site tumor nodules because of implantation of tumor cells after extraction of the gallbladder through an unprotected wound.
Tissue reduction enables extraction through small wounds but can be used only for benign specimens. Tissue reduction can be carried out by various techniques, including mechanical fragmentation and morcellation. It should be done inside a rip-proof bag whenever possible. This is essential for laparoscopic splenectomy to prevent implantation of splenic fragments on the serosal surfaces, which leads to selenosis. Most commonly the resected tissue should be hidden under the port and then everything should come together with the port. This technique is used for most of the small size organs like the appendix, gallbladder, small ovarian cyst, ectopic pregnancy, salpingectomy, small oophorectomy, etc.
Endobags
In some cases, the tissue to be removed is first encased in a specimen retrieval bag. These tissue retrieval bags are available in the market and can be prepared by the surgeon himself at the time of laparoscopic surgery. For infected tissue and in case of suspected carcinoma, tissue retrieval bag should be used. Many sizes of disposable tissue retrieval bags are available and hard rim of these retrieval bags is easy to negotiate inside the abdominal cavity. One can easily make the retrieval bag by tying and cutting the fingers of sterilized gloves. If the gloves used for the retrieval of tissue, it should be used carefully. It should not puncture while removing from the abdominal cavity.
Disposable endobags
Endobags
The glove is kept stretched while one assistant will tie it in the middle. Keeping it stretched will create a good dumbbell after knotting and so there is no chance of slipping of knot inside the abdominal cavity. The latex material used to manufacture gloves sometimes, react with human tissue and it can create a problem if the glove is punctured and a piece of latex is left inside the human body. Most commonly this torn piece of gloves can be missed in the layers of the abdominal wall. At the time of the introduction of glove endobag, it should be held by its cut end and kept stretched over the shaft of grasper to decrease its thickness. The polythene covering of ryels tube can also be used as an inexpensive readymade retrieval bag. This is sterilized and open at one end. These polythene bags can be used as an excellent retrieval pouch if used carefully. The polythene bags have one demerit that sometimes the edges are difficult to find out because it is transparent and secondly because it is thin and does not have an elastic property like gloves so it slips easily after once held by the grasper. The drawback of this self-made retrieval bag is that they do not have hard ream so it is difficult to manipulate inside the abdominal cavity. These bags can be introduced inside the abdominal cavity through 10 mm ports. In special circumstances, if there is difficulty is found it can be introduced directly through the port wound after withdrawing the cannula. Once the retrieval bag is inside it should be positioned in free abdominal space and the rim of the bag should be stabilized with nondominant hand and the dominant hand should be used to put the specimen inside. Once the bag is inside the abdominal cavity both the edges of the retrieval bag should be lifted to displace the specimen into the base of the bag. Condom can also be used for retrieving tissue. The lubricated condom should be avoided because it can cause tissue reaction. To take the specimen out, the surgeon should hide the mouth of the retrieval bag inside the cannula by pulling it and then the cannula together with the neck of the bag is pulled outside the abdominal cavity.
Once the neck of the bag is out, its opening is stretched with the help of an assistant. Ovum forceps can be introduced inside to morcellate the tissue manually if there is difficulty in pulling the bag out.
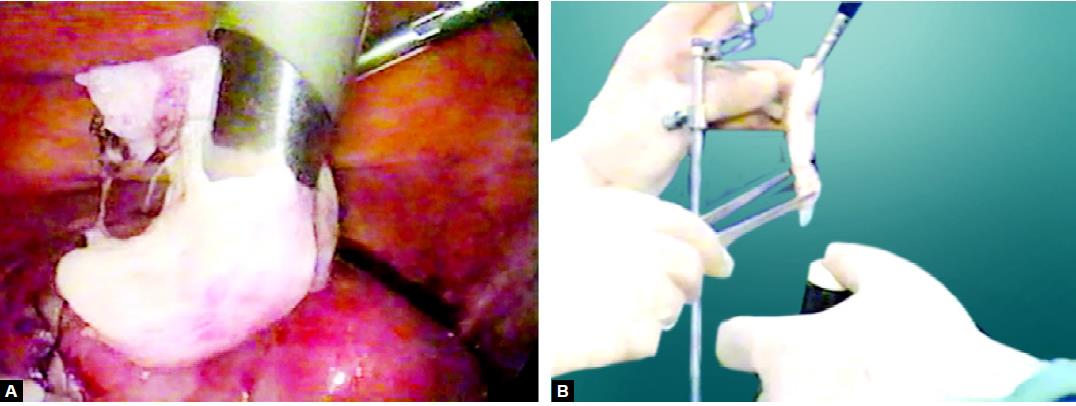
Making endobag with a glove
Glove endobag
Way of introducing endobag
Using glove endobag
Colpotomy
For large size gynecological tissue, the colpotomy route is good for retrieval. Colpotomy can be done laparoscopically with the help of a heal of the hook. Counter pushing by other instruments is effective. Sponge over sponge holding forceps is inserted in posterior vaginal fornix by one assistant and the surgeon cuts the vaginal fascia between both the uterosacral ligaments with the heel of the hook.
Hand-Assisted Laparoscopic Surgery
The hand-assisted technique was initially started keeping inside the ease of tissue retrievals, wherein the surgeon uses his or her hand, inserted through the initial incision, to aid in the exploration, isolation, and removal of tissue. The hand-assisted technique offers distinct advantages, the superior visualization afforded by the laparoscope, and a tactile component that is important in many aspects of surgery and has allowed surgeons to apply a less invasive approach to surgeries that previously could not have been done laparoscopically. Hand-assisted laparoscopy can also serve as a bridge between open surgery and straight laparoscopy, making it easier for surgeons to practice and learn the skills necessary for performing laparoscopic procedures.
Morcellator
The use of a morcellator is another way that facilitates the grinding of solid tissue and then these can be taken out without any difficulty. Recently many companies have launched a battery-operated morcellator. The morcellator is an important instrument for tissue retrieval in myomectomy and splenectomy. One of the early concerns about laparoscopic procedures in cancer patients was that they caused port site metastases, i.e. the appearance of recurrent tumor tissue at the site of trocar entry.
Electrical morcellator
Different type of morcellator
Morcellation of tissue
Cancer surgery, however, poses some unique challenges that make the application of laparoscopic surgery in oncology more problematic. It is critically important in cancer that whole organs should be removed intact (en bloc) so that pathologists can properly examine them and measure and document the depths and margins of tumor invasion. A second concern for surgical oncologists is cell transfer or cell spillage. Diseased tissue must be removed without contaminating adjacent tissues and structures with cancer cells. Because of these concerns, tissue morcellation, a technique commonly used in noncancer laparoscopic surgery in which the tissue is divided into pieces so that it can be removed more easily should not be used for oncologic procedures. All the 10 mm or greater than 10 mm defects should be closed properly to prevent any future possibility of a hernia. The suture passer should be used to pass the thread and then it should be tied externally. Especially, designed port closure instruments are also available commercially. If the port is suddenly taken out, the chances of port site hernia and adhesion are much higher. It is a good practice to insert some blunt instrument while removing the last port out, to prevent entrapment of omentum or bowel content. After closing the rectus sheath the skin can be closed by intradermal, skin stapler, or by any of the surgical skin glues available.




