Retroperitoneoscopy
Traditionally, laparoscopic surgeries are performed by transperitoneal approach following establishment of pneumoperitoneum by closed technique using the Veress needle or by the open mini-laparotomy. The parietal peritoneum is then secondarily incised and dissected to obtain access to the retroperitoneal target organs like kidneys, ureters, adrenals, and lymph nodes. Transperitoneal laparoscopy, although seemingly expeditious, invites the potential calamities of possible vascular and bowel injuries. On the other hand, retroperitoneal laparoscopy has its own difficulty due to working in a contained limited space. However, with technical refinements, several recent reports of successful retroperitoneoscopic surgeries have proved the feasibility and distinct advantages of this approach.
Historical Perspective
Retroperitoneoscopy has experienced a delayed development and acceptance compared with peritoneoscopy. Difficulties in providing adequate visualization and room for surgical maneuvering as well as concerns about deleterious effects of insufflating the retroperitoneal space account for this retarded progression. Although pneumoretroperitoneum has been used safely for more than 50 years to aid in radiographic visualization of the kidneys and adrenals, the conjunctive use of endoscopes has only recently been attempted. Retroperitoneoscopy through the flank in a human was pioneered by Wickham, who performed an extra-peritoneal laparoscopic ureterolithotomy in 1978.
Earliest techniques, termed pelviscopy, utilized a telescope to bluntly dissect within the pelvic retroperitoneum to sample pelvic lymph nodes. The obvious disadvantage of such technique has been the difficulty in exposing the obturator nodes, precluding the performance of an adequate staging lymphadenectomy. In the initial series reported by Hald and Rasmussen, many of the patients had no lymph nodes found in their surgical specimen. With refinements of surgical techniques, subsequently more complete pelviscopic node dissections have been reported.
Surgical Technique
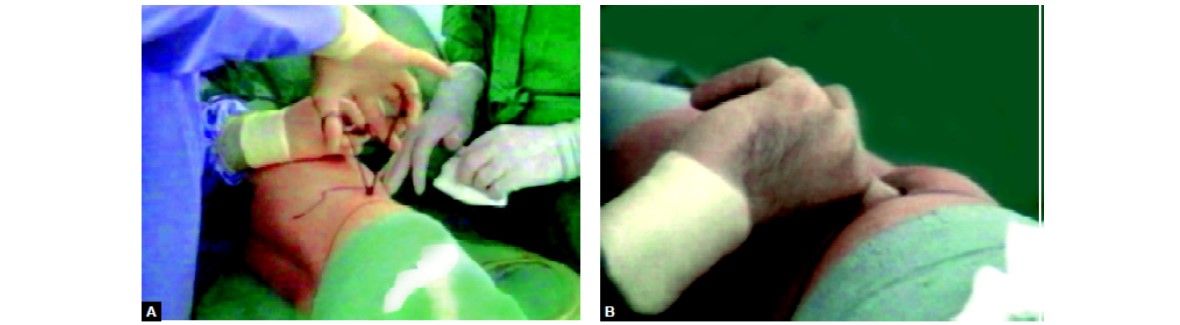
Probably the most important initial step in retroperitoneoscopy is the expansion and distention of the retroperitoneal space by an expanding balloon device. A balloon device modified fingers of a latex rubber glove is tied off, and the glove is secured over the distal end of the sheath of cannula. The device is placed in the retroperitoneum and expanded by injecting saline. Special trocars are available with transparent balloons at their inner end that can be inflated with air or fluid to allow laparoscopic visibility of retroperitoneum through the clear distended balloon.

Finger of glove over sheath of cannula
Retroperitoneoscopy through the Flank
This approach is applicable to surgery on adrenals, kidneys, and upper ureters. The patient is placed in a lateral decubitus position with slight forward tilt. A small incision is made about 2 cm below the twelfth rib, just lateral to the sacrospinalis. The incision is deepened through the fused lamellae of lumbar fascia to enter the perinephric space. The space is further dissected by blunt digital exploration. The expanding device is introduced into the retroperitoneal space and about 800-1000 ml saline are injected to inflate the balloon. The balloon is then deflated and removed. Laparoscope in 11 mm trocar is introduced into the retroperitoneal space and carbon dioxide insufflation is continued to maintain a pressure of about 14 mm Hg. With the posterior parietal peritoneum pushed away by the expanding device, the retroperitoneal space is widely opened by continued insufflation, and subsequent working ports are established under camera vision. The number and location of accessory ports are determined by the surgical procedure to be undertaken. However, it is usually advisable to keep the ports posterior to the anterior axillary line to avoid puncture of the lateral peritoneal reflection. During laparoscopic dissection it is often helpful to move the laparoscope to the anterior ports for better visibility as the situation may dictate.

Place for primary trocar insertion in retroperitoneoscopy
Finger dissection of retroperitoneal space
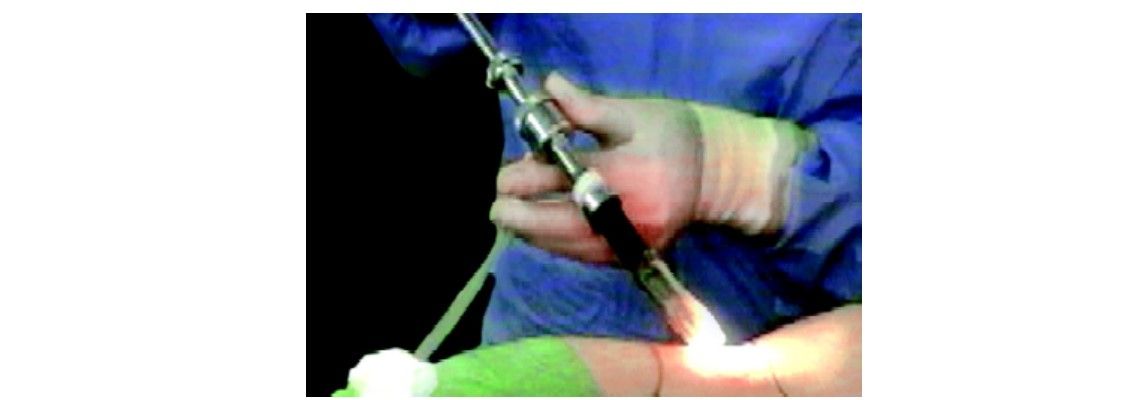
Laparoscope with balloon cannula system
Retroperitoneoscopy: Anterolateral
For surgery on mid and lower ureters and for internal spermatic vein ligation, the retroperitoneoscopy is performed by a small incision at McBurney’s point. The external oblique aponeurosis is incised, and underlying fibers of the internal oblique and transverse muscles of the abdomen are split to reach the extraperitoneal space. Following careful digital dissection, the expanding device is introduced and inflated in the retroperitoneum.
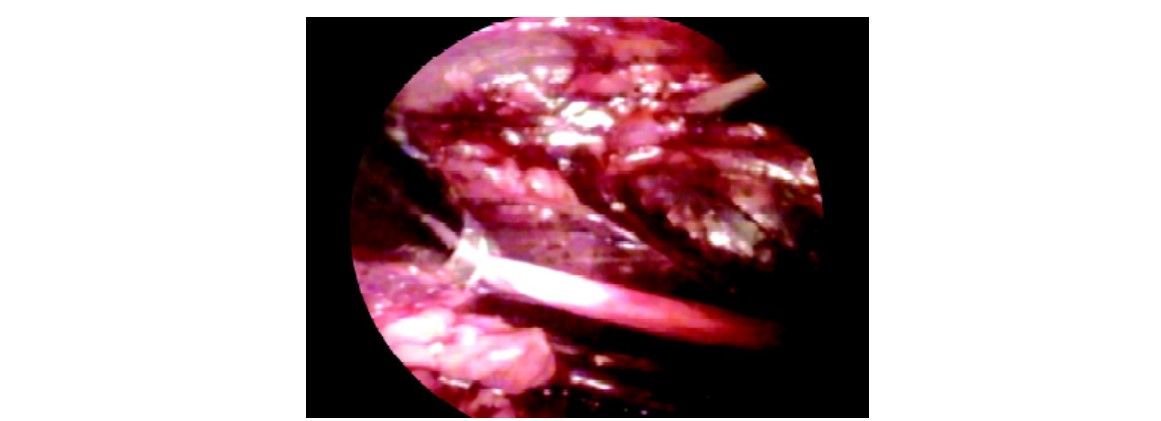
Ureter as seen during retroperitoneoscopy
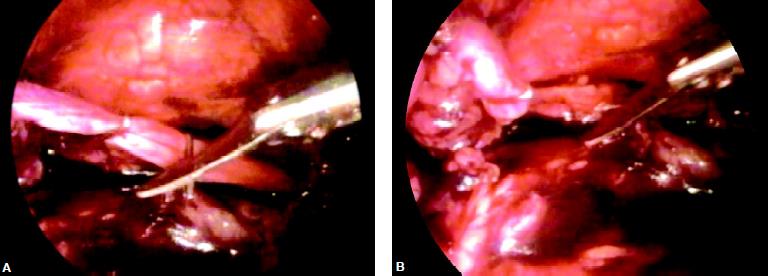
Two clips are applied over ureter and cut in between
Retroperitoneoscopy for Pelvic Lymph Node
Pelvic retroperitoneoscopy is ideal for bilateral staging pelvic lymph node dissection and bladder neck suspension procedures. A small midline incision is made about 2 cm below the umbilicus. The linea alba is opened, and underlying extraperitoneal space is developed by digital dissection behind the rectus muscle of the abdomen. The expanding device is introduced and expanded by injecting about 1200 ml saline solution. The balloon is decompressed and re-moved. The laparoscope is introduced with high-flow carbon dioxide insufflation. Anatomic landmarks of the symphysis pubis, superior pubic rami, bladder neck, and external iliac vein pulsations in the pelvis are easily identified. Complete bilateral staging lymph-adenectomy is accomplished by en bloc dissection of the fibrofatty lymphatic tissue from the triangular area bounded laterally by the external iliac vein, proximally by the hypogastric artery, and inferiorly by the endopelvic fascia.
Posterior dissection of left kidney
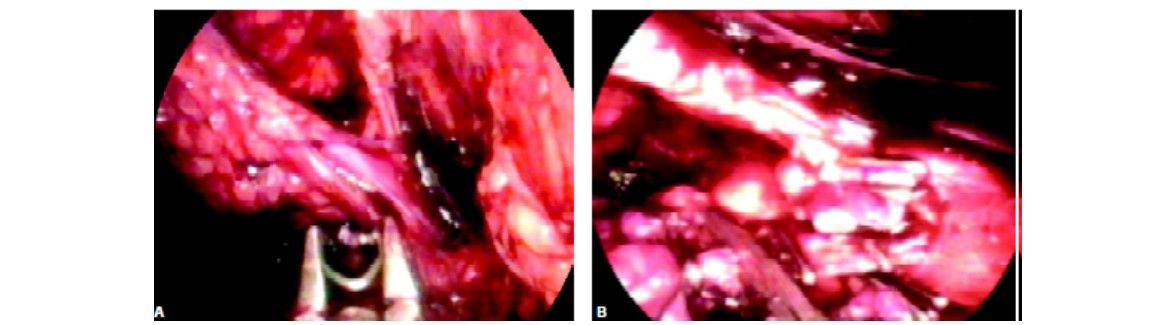
Dissection of hilum of kidney and application of clips before cutting
Conclusion
The pioneering concept of retroperitoneal expansion by Gaur and coworkers has led to the resurgence of retroperitoneoscopy. Artificial balloon expansion creates the necessary space and retraction of neighboring viscera, so that subsequent insufflation can maintain the open space for surgical maneuvering. In a way, this technique simulates the steps of dissection and retraction traditionally used during open surgery.
Aside from preventing the potential hazards of trans- peritoneal access and intraperitoneal dissection, there are certain distinct advantages of retroperitoneoscopy in patient positioning, intestinal retraction, anatomic approach to the renal hilum, and postoperative wound drainage. For retroperitoneal approaches to the adrenals, kidneys, and ureters the patient is placed in the lateral decubitus position, as opposed to the supine position for laparoscopy. The intestines contained within the intact peritoneal envelope remain displaced during retroperitoneal dissection, thereby avoiding extensive colonic mobilization and constant retraction of bowel. During nephrectomy, the renal hilum is approached from the posterior aspect, allowing easier initial control of the renal arteries. Similarly exposure of other retroperitoneal structures such as the adrenal gland in the right side is relatively easier than with the anterior approach. The closed extraperitoneal space allows more effective postoperative drainage, especially following reconstructive and reparative surgery such as pyeloplasty, partial nephrectomy, pyelolithotomy, and ureterolithotomy. The perceived difficulties of surgical dissection of kidneys and adrenal glands in a restricted environment during retroperitoneoscopy has not proved true with the present technique or initial balloon expansion. However, organ entrapment, especially of large specimens, in the limited space is difficult. The anterolateral extraperitoneal approach allows access for ureterolithotomy on the lower ureter at and above the pelvic inlet. Internal spermatic vein ligation extraperitoneally is done for treatment of varicocele. The extraperitoneal dissection appears, however, to be more extensive, and such an approach will not be suitable for bilateral variocele surgery. In the pelvis, the excellent anatomic appearance of the bladder, bladder neck, and symphysial structures makes the extraperitoneal approach ideally suited for procedures such as laparoscopic bladder-neck suspension and surgery for urachal pathologies. The majority of bladder diverticula are located posterolaterally and are therefore not often amenable to extraperitoneal excision. For the bilateral staging pelvic lymphadenectomy the extraperitoneal approach has proved its safety and feasibility. The lymph node dissection is anatomically precise, simulating the standards of open pelvic lymphadenectomy. The advantage of retroperitoneal CO2 insufflation is that by avoiding CO2 contact with the peritoneal membrane, there is less hypothermia and reduced postoperative pain from diaphragmatic irritation. In conclusion, retroperitoneoscopy offers another viable option in the developing field of laparoscopy. The surgical indications that warrant an extraperitoneal approach in open surgery hold true for retroperitoneoscopy as well. As a minimally invasive technique, retroperitoneoscopy emulates the established standards and principles of open urologic procedures without compromising surgical efficiency and patient safety.




