
Page 36 - World Journal of Laparoscopic Surgeons
P. 36
WJOLS
Posterior Rectus Sheath
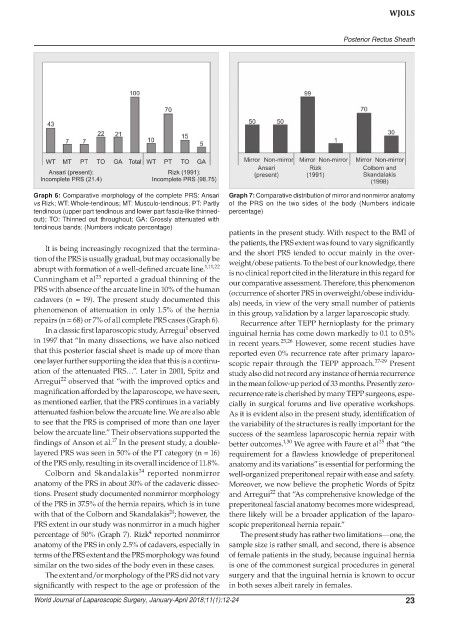
Graph 6: Comparative morphology of the complete PRS: Ansari Graph 7: Comparative distribution of mirror and nonmirror anatomy
vs Rizk; WT: Whole-tendinous; MT: Musculo-tendinous; PT: Partly of the PRS on the two sides of the body (Numbers indicate
tendinous (upper part tendinous and lower part fascia-like thinned- percentage)
out); TO: Thinned out throughout; GA: Grossly attenuated with
tendinous bands; (Numbers indicate percentage)
patients in the present study. With respect to the BMI of
the patients, the PRS extent was found to vary significantly
It is being increasingly recognized that the termina- and the short PRS tended to occur mainly in the over-
tion of the PRS is usually gradual, but may occasionally be weight/obese patients. To the best of our knowledge, there
abrupt with formation of a well-defined arcuate line. 1,11,22 is no clinical report cited in the literature in this regard for
23
Cunningham et al reported a gradual thinning of the our comparative assessment. Therefore, this phenomenon
PRS with absence of the arcuate line in 10% of the human (occurrence of shorter PRS in overweight/obese individu-
cadavers (n = 19). The present study documented this als) needs, in view of the very small number of patients
phenomenon of attenuation in only 1.5% of the hernia in this group, validation by a larger laparoscopic study.
repairs (n = 68) or 7% of all complete PRS cases (Graph 6). Recurrence after TEPP hernioplasty for the primary
1
In a classic first laparoscopic study, Arregui observed inguinal hernia has come down markedly to 0.1 to 0.5%
in 1997 that “In many dissections, we have also noticed in recent years. 25,26 However, some recent studies have
that this posterior fascial sheet is made up of more than reported even 0% recurrence rate after primary laparo-
one layer further supporting the idea that this is a continu- scopic repair through the TEPP approach. 27-29 Present
ation of the attenuated PRS…”. Later in 2001, Spitz and study also did not record any instance of hernia recurrence
22
Arregui observed that “with the improved optics and in the mean follow-up period of 33 months. Presently zero-
magnification afforded by the laparoscope, we have seen, recurrence rate is cherished by many TEPP surgeons, espe-
as mentioned earlier, that the PRS continues in a variably cially in surgical forums and live operative workshops.
attenuated fashion below the arcuate line. We are also able As it is evident also in the present study, identification of
to see that the PRS is comprised of more than one layer the variability of the structures is really important for the
below the arcuate line.” Their observations supported the success of the seamless laparoscopic hernia repair with
17
findings of Anson et al. In the present study, a double- better outcomes. 1,30 We agree with Faure et al that “the
25
layered PRS was seen in 50% of the PT category (n = 16) requirement for a flawless knowledge of preperitoneal
of the PRS only, resulting in its overall incidence of 11.8%. anatomy and its variations” is essential for performing the
24
Colborn and Skandalakis reported nonmirror well-organized preperitoneal repair with ease and safety.
anatomy of the PRS in about 30% of the cadaveric dissec- Moreover, we now believe the prophetic Words of Spitz
22
tions. Present study documented nonmirror morphology and Arregui that “As comprehensive knowledge of the
of the PRS in 37.5% of the hernia repairs, which is in tune preperitoneal fascial anatomy becomes more widespread,
24
with that of the Colborn and Skandalakis ; however, the there likely will be a broader application of the laparo-
PRS extent in our study was nonmirror in a much higher scopic preperitoneal hernia repair.”
4
percentage of 50% (Graph 7). Rizk reported nonmirror The present study has rather two limitations—one, the
anatomy of the PRS in only 2.5% of cadavers, especially in sample size is rather small, and second, there is absence
terms of the PRS extent and the PRS morphology was found of female patients in the study, because inguinal hernia
similar on the two sides of the body even in these cases. is one of the commonest surgical procedures in general
The extent and/or morphology of the PRS did not vary surgery and that the inguinal hernia is known to occur
significantly with respect to the age or profession of the in both sexes albeit rarely in females.
World Journal of Laparoscopic Surgery, January-April 2018;11(1):12-24 23