
Page 29 - World Journal of Laparoscopic Surgeons
P. 29
Maulana M Ansari
A B
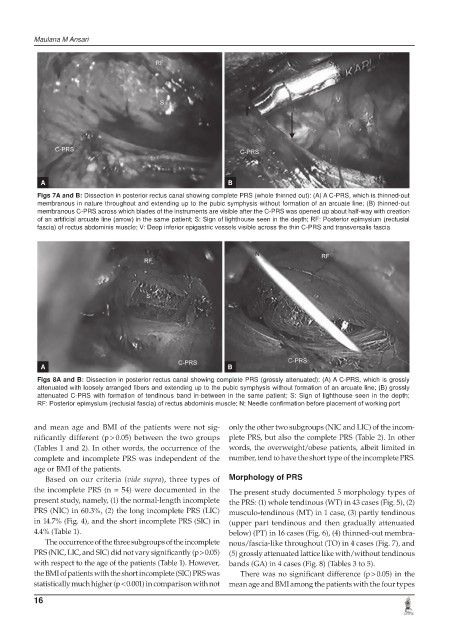
Figs 7A and B: Dissection in posterior rectus canal showing complete PRS (whole thinned out): (A) A C-PRS, which is thinned-out
membranous in nature throughout and extending up to the pubic symphysis without formation of an arcuate line; (B) thinned-out
membranous C-PRS across which blades of the instruments are visible after the C-PRS was opened up about half-way with creation
of an artificial arcuate line (arrow) in the same patient; S: Sign of lighthouse seen in the depth; RF: Posterior epimysium (rectusial
fascia) of rectus abdominis muscle; V: Deep inferior epigastric vessels visible across the thin C-PRS and transversalis fascia
A B
Figs 8A and B: Dissection in posterior rectus canal showing complete PRS (grossly attenuated): (A) A C-PRS, which is grossly
attenuated with loosely arranged fibers and extending up to the pubic symphysis without formation of an arcuate line; (B) grossly
attenuated C-PRS with formation of tendinous band in-between in the same patient; S: Sign of lighthouse seen in the depth;
RF: Posterior epimysium (rectusial fascia) of rectus abdominis muscle; N: Needle confirmation before placement of working port
and mean age and BMI of the patients were not sig- only the other two subgroups (NIC and LIC) of the incom-
nificantly different (p > 0.05) between the two groups plete PRS, but also the complete PRS (Table 2). In other
(Tables 1 and 2). In other words, the occurrence of the words, the overweight/obese patients, albeit limited in
complete and incomplete PRS was independent of the number, tend to have the short type of the incomplete PRS.
age or BMI of the patients.
Based on our criteria (vide supra), three types of Morphology of PRS
the incomplete PRS (n = 54) were documented in the The present study documented 5 morphology types of
present study, namely, (1) the normal-length incomplete the PRS: (1) whole tendinous (WT) in 43 cases (Fig. 5), (2)
PRS (NIC) in 60.3%, (2) the long incomplete PRS (LIC) musculo-tendinous (MT) in 1 case, (3) partly tendinous
in 14.7% (Fig. 4), and the short incomplete PRS (SIC) in (upper part tendinous and then gradually attenuated
4.4% (Table 1). below) (PT) in 16 cases (Fig. 6), (4) thinned-out membra-
The occurrence of the three subgroups of the incomplete nous/fascia-like throughout (TO) in 4 cases (Fig. 7), and
PRS (NIC, LIC, and SIC) did not vary significantly (p > 0.05) (5) grossly attenuated lattice like with/without tendinous
with respect to the age of the patients (Table 1). However, bands (GA) in 4 cases (Fig. 8) (Tables 3 to 5).
the BMI of patients with the short incomplete (SIC) PRS was There was no significant difference (p > 0.05) in the
statistically much higher (p < 0.001) in comparison with not mean age and BMI among the patients with the four types
16