
Page 52 - Journal of Laparoscopic Surgery
P. 52
Vimal K Jain et al.
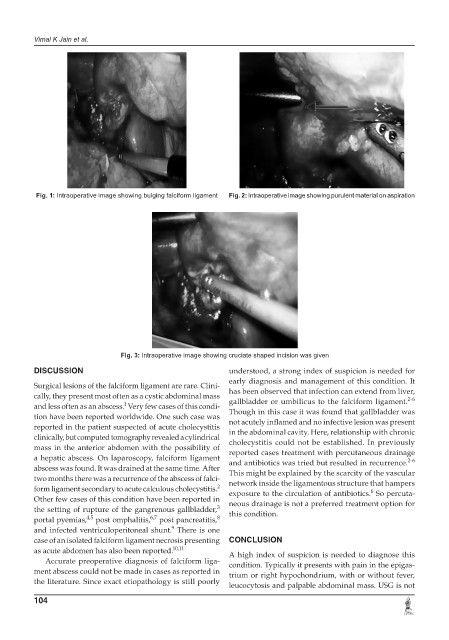
Fig. 1: Intraoperative image showing bulging falciform ligament Fig. 2: Intraoperative image showing purulent material on aspiration
Fig. 3: Intraoperative image showing cruciate shaped incision was given
DISCUSSION understood, a strong index of suspicion is needed for
early diagnosis and management of this condition. It
Surgical lesions of the falciform ligament are rare. Clini- has been observed that infection can extend from liver,
cally, they present most often as a cystic abdominal mass 2-6
1
and less often as an abscess. Very few cases of this condi- gallbladder or umbilicus to the falciform ligament.
Though in this case it was found that gallbladder was
tion have been reported worldwide. One such case was not acutely inflamed and no infective lesion was present
reported in the patient suspected of acute cholecystitis in the abdominal cavity. Here, relationship with chronic
clinically, but computed tomography revealed a cylindrical cholecystitis could not be established. In previously
mass in the anterior abdomen with the possibility of reported cases treatment with percutaneous drainage
a hepatic abscess. On laparoscopy, falciform ligament and antibiotics was tried but resulted in recurrence.
2-6
abscess was found. It was drained at the same time. After This might be explained by the scarcity of the vascular
two months there was a recurrence of the abscess of falci- network inside the ligamentous structure that hampers
2
form ligament secondary to acute calculous cholecystitis. exposure to the circulation of antibiotics. So percuta-
6
Other few cases of this condition have been reported in neous drainage is not a preferred treatment option for
3
the setting of rupture of the gangrenous gallbladder, this condition.
4,5
6,7
portal pyemias, post omphalitis, post pancreatitis, 8
9
and infected ventriculoperitoneal shunt. There is one
case of an isolated falciform ligament necrosis presenting CONCLUSION
as acute abdomen has also been reported. 10,11 A high index of suspicion is needed to diagnose this
Accurate preoperative diagnosis of falciform liga- condition. Typically it presents with pain in the epigas-
ment abscess could not be made in cases as reported in trium or right hypochondrium, with or without fever,
the literature. Since exact etiopathology is still poorly
leucocytosis and palpable abdominal mass. USG is not
104