
Page 46 - World Journal of Laparoscopic Surgery
P. 46
Laparoscopy in Unusual Abdominal Emergencies: Report and Review
Figs 4A and B: (A) Stomach herniating through defect 4; (B) Defect after reduction of content
Figs 5A and B: Intraoperative findings. (A) Hemoperitoneum 5; (B) Splenic laceration with ongoing bleed
expanded to unusual conditions apart from acute appendicitis,
hollow viscus perforation, and obstruction.
Over the last three decades, a number of studies have reported
its role in diagnosis with accuracy rates of between 86–100%, 6–8
and with accumulated surgical experience and skills a large
number of patients managed exclusively with a laparoscopic
approach. 9,10 Its role has come a big way in selected patients with
penetrating abdominal trauma who are hemodynamically stable
as in a large number of cases, there is no peritoneal breach, and
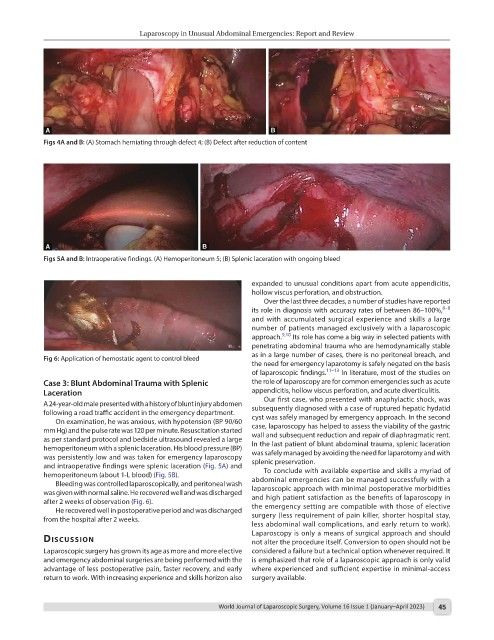
Fig 6: Application of hemostatic agent to control bleed
the need for emergency laparotomy is safely negated on the basis
of laparoscopic findings. 11–13 In literature, most of the studies on
Case 3: Blunt Abdominal Trauma with Splenic the role of laparoscopy are for common emergencies such as acute
Laceration appendicitis, hollow viscus perforation, and acute diverticulitis.
A 24-year-old male presented with a history of blunt injury abdomen Our first case, who presented with anaphylactic shock, was
following a road traffic accident in the emergency department. subsequently diagnosed with a case of ruptured hepatic hydatid
On examination, he was anxious, with hypotension (BP 90/60 cyst was safely managed by emergency approach. In the second
mm Hg) and the pulse rate was 120 per minute. Resuscitation started case, laparoscopy has helped to assess the viability of the gastric
as per standard protocol and bedside ultrasound revealed a large wall and subsequent reduction and repair of diaphragmatic rent.
hemoperitoneum with a splenic laceration. His blood pressure (BP) In the last patient of blunt abdominal trauma, splenic laceration
was persistently low and was taken for emergency laparoscopy was safely managed by avoiding the need for laparotomy and with
and intraoperative findings were splenic laceration (Fig. 5A) and splenic preservation.
hemoperitoneum (about 1-L blood) (Fig. 5B). To conclude with available expertise and skills a myriad of
Bleeding was controlled laparoscopically, and peritoneal wash abdominal emergencies can be managed successfully with a
was given with normal saline. He recovered well and was discharged laparoscopic approach with minimal postoperative morbidities
after 2 weeks of observation (Fig. 6). and high patient satisfaction as the benefits of laparoscopy in
He recovered well in postoperative period and was discharged the emergency setting are compatible with those of elective
from the hospital after 2 weeks. surgery (less requirement of pain killer, shorter hospital stay,
less abdominal wall complications, and early return to work).
Laparoscopy is only a means of surgical approach and should
dIscussIon not alter the procedure itself. Conversion to open should not be
Laparoscopic surgery has grown its age as more and more elective considered a failure but a technical option whenever required. It
and emergency abdominal surgeries are being performed with the is emphasized that role of a laparoscopic approach is only valid
advantage of less postoperative pain, faster recovery, and early where experienced and sufficient expertise in minimal-access
return to work. With increasing experience and skills horizon also surgery available.
World Journal of Laparoscopic Surgery, Volume 16 Issue 1 (January–April 2023) 45