
Page 36 - World Journal of Laparoscopic Surgery
P. 36
Hemorrhoidectomy by MIPH
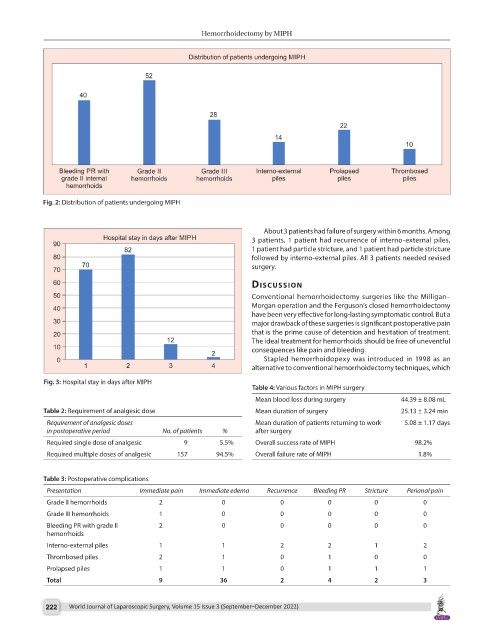
Fig. 2: Distribution of patients undergoing MIPH
About 3 patients had failure of surgery within 6 months. Among
3 patients, 1 patient had recurrence of interno-external piles,
1 patient had particle stricture, and 1 patient had particle stricture
followed by interno-external piles. All 3 patients needed revised
surgery.
dIscussIon
Conventional hemorrhoidectomy surgeries like the Milligan–
Morgan operation and the Ferguson’s closed hemorrhoidectomy
have been very effective for long-lasting symptomatic control. But a
major drawback of these surgeries is significant postoperative pain
that is the prime cause of detention and hesitation of treatment.
The ideal treatment for hemorrhoids should be free of uneventful
consequences like pain and bleeding.
Stapled hemorrhoidopexy was introduced in 1998 as an
alternative to conventional hemorrhoidectomy techniques, which
Fig. 3: Hospital stay in days after MIPH
Table 4: Various factors in MIPH surgery
Mean blood loss during surgery 44.39 ± 8.08 mL
Table 2: Requirement of analgesic dose Mean duration of surgery 25.13 ± 3.24 min
Requirement of analgesic doses Mean duration of patients returning to work 5.08 ± 1.17 days
in postoperative period No. of patients % after surgery
Required single dose of analgesic 9 5.5% Overall success rate of MIPH 98.2%
Required multiple doses of analgesic 157 94.5% Overall failure rate of MIPH 1.8%
Table 3: Postoperative complications
Presentation Immediate pain Immediate edema Recurrence Bleeding PR Stricture Perianal pain
Grade II hemorrhoids 2 0 0 0 0 0
Grade III hemorrhoids 1 0 0 0 0 0
Bleeding PR with grade II 2 0 0 0 0 0
hemorrhoids
Interno-external piles 1 1 2 2 1 2
Thrombosed piles 2 1 0 1 0 0
Prolapsed piles 1 1 0 1 1 1
Total 9 36 2 4 2 3
222 World Journal of Laparoscopic Surgery, Volume 15 Issue 3 (September–December 2022)