
Page 30 - World Journal of Laparoscopic Surgery
P. 30
Laparoscopic Ventral Rectopexy for Rectal Prolapse
2015 to 2017 obtaining ethical approval from the local ethical dissection continues downward in the midpoint between the
committee and after taking fully informed consent from patients. rectum and sidewall to the level of the pelvic floor. Dissection is
performed in the anterior space through Denonvilliers’ fascia to
Patient Selection and Evaluation the rectovaginal space. In men, the dissection in the recto-vesical
This study included 20 patients with CRP who underwent LVMR pouch is carried to the apex of the prostate but the lateral dissection
with polypropylene mesh. around the seminal vesicles is avoided. In some cases, the hernia sac
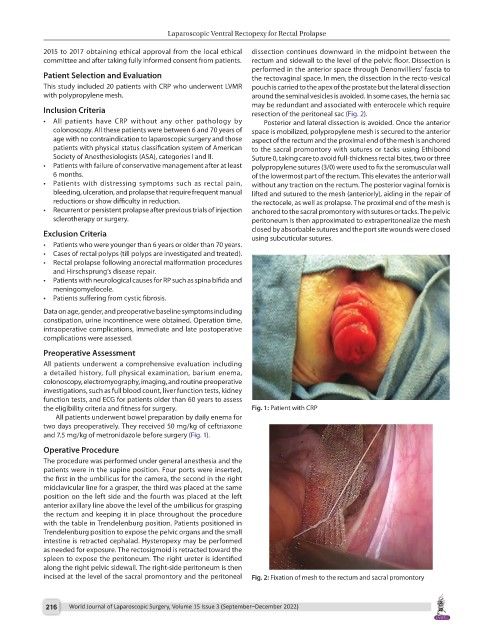
may be redundant and associated with enterocele which require
Inclusion Criteria resection of the peritoneal sac (Fig. 2).
• All patients have CRP without any other pathology by Posterior and lateral dissection is avoided. Once the anterior
colonoscopy. All these patients were between 6 and 70 years of space is mobilized, polypropylene mesh is secured to the anterior
age with no contraindication to laparoscopic surgery and those aspect of the rectum and the proximal end of the mesh is anchored
patients with physical status classification system of American to the sacral promontory with sutures or tacks using Ethibond
Society of Anesthesiologists (ASA), categories I and II. Suture 0, taking care to avoid full-thickness rectal bites, two or three
• Patients with failure of conservative management after at least polypropylene sutures (3/0) were used to fix the seromuscular wall
6 months. of the lowermost part of the rectum. This elevates the anterior wall
• Patients with distressing symptoms such as rectal pain, without any traction on the rectum. The posterior vaginal fornix is
bleeding, ulceration, and prolapse that require frequent manual lifted and sutured to the mesh (anteriorly), aiding in the repair of
reductions or show difficulty in reduction. the rectocele, as well as prolapse. The proximal end of the mesh is
• Recurrent or persistent prolapse after previous trials of injection anchored to the sacral promontory with sutures or tacks. The pelvic
sclerotherapy or surgery. peritoneum is then approximated to extraperitonealize the mesh
closed by absorbable sutures and the port site wounds were closed
Exclusion Criteria using subcuticular sutures.
• Patients who were younger than 6 years or older than 70 years.
• Cases of rectal polyps (till polyps are investigated and treated).
• Rectal prolapse following anorectal malformation procedures
and Hirschsprung’s disease repair.
• Patients with neurological causes for RP such as spina bifida and
meningomyelocele.
• Patients suffering from cystic fibrosis.
Data on age, gender, and preoperative baseline symptoms including
constipation, urine incontinence were obtained. Operation time,
intraoperative complications, immediate and late postoperative
complications were assessed.
Preoperative Assessment
All patients underwent a comprehensive evaluation including
a detailed history, full physical examination, barium enema,
colonoscopy, electromyography, imaging, and routine preoperative
investigations, such as full blood count, liver function tests, kidney
function tests, and ECG for patients older than 60 years to assess
the eligibility criteria and fitness for surgery. Fig. 1: Patient with CRP
All patients underwent bowel preparation by daily enema for
two days preoperatively. They received 50 mg/kg of ceftriaxone
and 7.5 mg/kg of metronidazole before surgery (Fig. 1).
Operative Procedure
The procedure was performed under general anesthesia and the
patients were in the supine position. Four ports were inserted,
the first in the umbilicus for the camera, the second in the right
midclavicular line for a grasper, the third was placed at the same
position on the left side and the fourth was placed at the left
anterior axillary line above the level of the umbilicus for grasping
the rectum and keeping it in place throughout the procedure
with the table in Trendelenburg position. Patients positioned in
Trendelenburg position to expose the pelvic organs and the small
intestine is retracted cephalad. Hysteropexy may be performed
as needed for exposure. The rectosigmoid is retracted toward the
spleen to expose the peritoneum. The right ureter is identified
along the right pelvic sidewall. The right-side peritoneum is then
incised at the level of the sacral promontory and the peritoneal Fig. 2: Fixation of mesh to the rectum and sacral promontory
216 World Journal of Laparoscopic Surgery, Volume 15 Issue 3 (September–December 2022)