
Page 14 - World Journal of Laparoscopic Surgery
P. 14
Comparative Study of the Effect of Various Bariatric Surgery Methods
patients undergoing one of the following surgeries: classical bypass,
sleeve, and gastric bypasses with anastomosis, or not undergoing
surgery for any reason and receiving diet and exercise regimen for
weight loss despite the indication for surgery. Exclusion criteria
included alcohol intake or consumption of one of the drugs,
including amiodarone, methotrexate, tamoxifen, prednisolone,
dexamethasone, haloperidol, chlorpromazine, fluphenazine,
perphenazine, terclooperazine, aripiprazole, clozapine, olanzapine,
quiathiazin, risperidone at any time before surgery, or being
suspected of autoimmune hepatitis, viral hepatitis, Wilson’s disease,
or hemochromatosis.
Data from each patient, including age, sex, BMI, type of surgery,
presence or absence of IFG or diabetes, laboratory parameters (AST,
ALT, AlP, Alb, Plt), and liver ultrasound, preoperative and 6 months
after the operation were obtained from the above-mentioned
database.
After examining the patients, 900 patients were finally enrolled
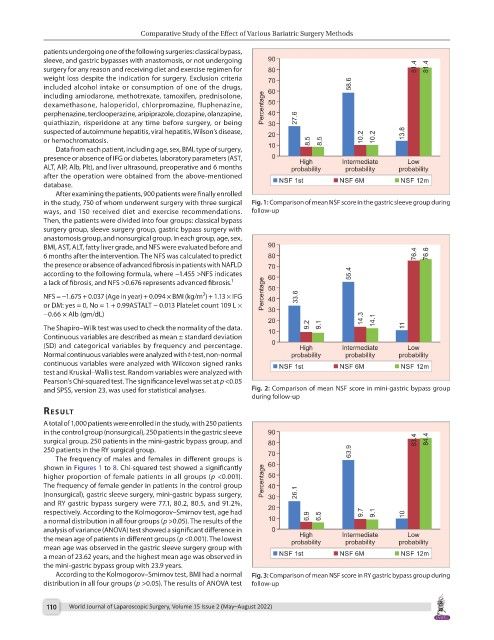
in the study, 750 of whom underwent surgery with three surgical Fig. 1: Comparison of mean NSF score in the gastric sleeve group during
ways, and 150 received diet and exercise recommendations. follow-up
Then, the patients were divided into four groups: classical bypass
surgery group, sleeve surgery group, gastric bypass surgery with
anastomosis group, and nonsurgical group. In each group, age, sex,
BMI, AST, ALT, fatty liver grade, and NFS were evaluated before and
6 months after the intervention. The NFS was calculated to predict
the presence or absence of advanced fibrosis in patients with NAFLD
according to the following formula, where −1.455 >NFS indicates
a lack of fibrosis, and NFS >0.676 represents advanced fibrosis. 1
2
NFS = −1.675 + 0.037 (Age in year) + 0.094 × BMI (kg/m ) + 1.13 × IFG
or DM: yes = 0, No = 1 + 0.99ASTALT − 0.013 Platelet count 109 L ×
−0.66 × Alb (gm/dL)
The Shapiro–Wilk test was used to check the normality of the data.
Continuous variables are described as mean ± standard deviation
(SD) and categorical variables by frequency and percentage.
Normal continuous variables were analyzed with t-test, non-normal
continuous variables were analyzed with Wilcoxon signed ranks
test and Kruskal–Wallis test. Random variables were analyzed with
Pearson’s Chi-squared test. The significance level was set at p <0.05
and SPSS, version 23, was used for statistical analyses. Fig. 2: Comparison of mean NSF score in mini-gastric bypass group
during follow-up
result
A total of 1,000 patients were enrolled in the study, with 250 patients
in the control group (nonsurgical), 250 patients in the gastric sleeve
surgical group, 250 patients in the mini-gastric bypass group, and
250 patients in the RY surgical group.
The frequency of males and females in different groups is
shown in Figures 1 to 8. Chi-squared test showed a significantly
higher proportion of female patients in all groups (p <0.001).
The frequency of female gender in patients in the control group
(nonsurgical), gastric sleeve surgery, mini-gastric bypass surgery,
and RY gastric bypass surgery were 77.1, 80.2, 80.5, and 91.2%,
respectively. According to the Kolmogorov–Smirnov test, age had
a normal distribution in all four groups (p >0.05). The results of the
analysis of variance (ANOVA) test showed a significant difference in
the mean age of patients in different groups (p <0.001). The lowest
mean age was observed in the gastric sleeve surgery group with
a mean of 23.62 years, and the highest mean age was observed in
the mini-gastric bypass group with 23.9 years.
According to the Kolmogorov–Smirnov test, BMI had a normal Fig. 3: Comparison of mean NSF score in RY gastric bypass group during
distribution in all four groups (p >0.05). The results of ANOVA test follow-up
110 World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022)