
Page 80 - World Journal of Laparoscopic Surgery
P. 80
A Prospective Observational Study on Single-incision or Conventional Three-port Laparoscopic TEP Inguinal Hernia Repair
with respect to the three-port conventional totally extraperitoneal dose were administered before the procedure in each patient.
(CTEP) repair in the management of groin hernias has not been Surgery was performed on a routine elective basis after proper
thoroughly published to date. 5–7 investigation as per following operative techniques.
Single-incision Totally Extraperitoneal Inguinal Hernia
MAterIAls And Methods Repair Technique
The study was a prospective observational study of patients with Under general anesthesia, the patient is placed supine with both
groin hernia (Fig. 1). There were two study groups. One group of arms adducted. Later the patient is placed in the Trendelenburg
patients has undergone single-incision totally extraperitoneal position with the side contralateral to the hernia site tilted down.
inguinal hernia repair technique and the other via three-port A 25-mm subumbilical incision is made, followed by dissection of
CTEP repair procedure. The two groups were then compared the subcutaneous tissue down to the rectus abdominis sheath. An
based on intraoperative and postoperative parameters. The main incision approximately 3 cm in length is made over the anterior
aim of the study was to observe these two techniques in terms rectus sheath and opened, blunt dissection using a finger or gauze is
of the following: performed between the rectus muscle and the posterior rectus sheath
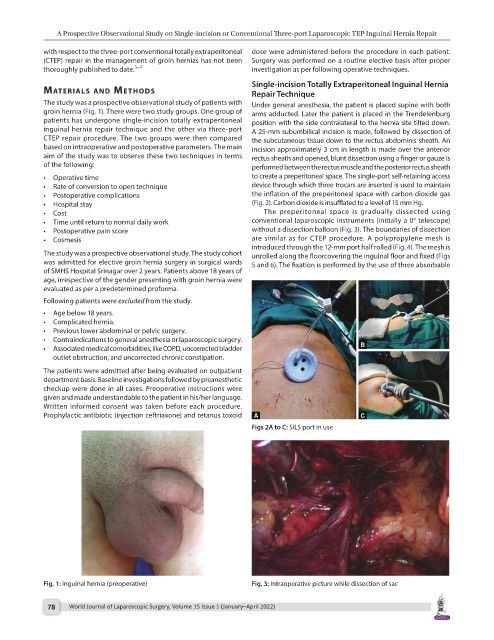
• Operative time to create a preperitoneal space. The single-port self-retaining access
• Rate of conversion to open technique device through which three trocars are inserted is used to maintain
• Postoperative complications the inflation of the preperitoneal space with carbon dioxide gas
• Hospital stay (Fig. 2). Carbon dioxide is insufflated to a level of 15 mm Hg.
• Cost The preperitoneal space is gradually dissected using
• Time until return to normal daily work conventional laparoscopic instruments (initially a 0° telescope)
• Postoperative pain score without a dissection balloon (Fig. 3). The boundaries of dissection
• Cosmesis are similar as for CTEP procedure. A polypropylene mesh is
introduced through the 12-mm port half rolled (Fig. 4). The mesh is
The study was a prospective observational study. The study cohort unrolled along the floorcovering the inguinal floor and fixed (Figs
was admitted for elective groin hernia surgery in surgical wards 5 and 6). The fixation is performed by the use of three absorbable
of SMHS Hospital Srinagar over 2 years. Patients above 18 years of
age, irrespective of the gender presenting with groin hernia were
evaluated as per a predetermined proforma.
Following patients were excluded from the study.
• Age below 18 years.
• Complicated hernia.
• Previous lower abdominal or pelvic surgery.
• Contraindications to general anesthesia or laparoscopic surgery.
• Associated medical comorbidities, like COPD, uncorrected bladder
outlet obstruction, and uncorrected chronic constipation.
The patients were admitted after being evaluated on outpatient
department basis. Baseline investigations followed by preanesthetic
checkup were done in all cases. Preoperative instructions were
given and made understandable to the patient in his/her language.
Written informed consent was taken before each procedure.
Prophylactic antibiotic (injection ceftriaxone) and tetanus toxoid
Figs 2A to C: SILS port in use
Fig. 1: Inguinal hernia (preoperative) Fig. 3: Intraoperative picture while dissection of sac
78 World Journal of Laparoscopic Surgery, Volume 15 Issue 1 (January–April 2022)