
Page 39 - tmp
P. 39
Incidental CaGB in Operated Cases of Gallstone Disease
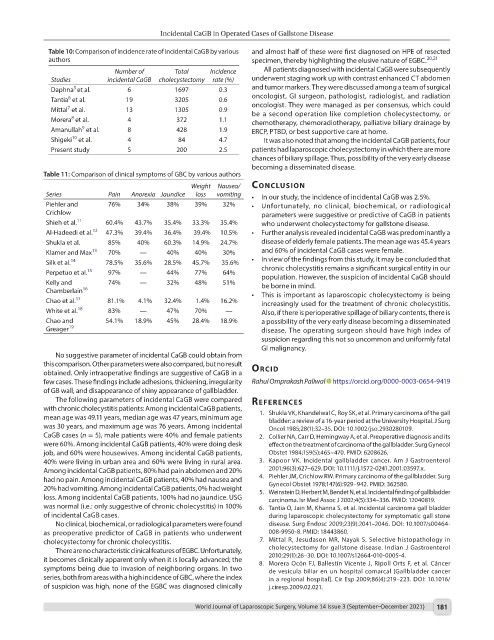
Table 10: Comparison of incidence rate of incidental CaGB by various and almost half of these were first diagnosed on HPE of resected
authors specimen, thereby highlighting the elusive nature of EGBC. 20,21
Number of Total Incidence All patients diagnosed with incidental CaGB were subsequently
Studies incidental CaGB cholecystectomy rate (%) underwent staging work up with contrast enhanced CT abdomen
5
Daphna et al. 6 1697 0.3 and tumor markers. They were discussed among a team of surgical
6
Tantia et al. 19 3205 0.6 oncologist, GI surgeon, pathologist, radiologist, and radiation
oncologist. They were managed as per consensus, which could
7
Mittal et al. 13 1305 0.9 be a second operation like completion cholecystectomy, or
8
Morera et al. 4 372 1.1 chemotherapy, chemoradiotherapy, palliative biliary drainage by
9
Amanullah et al. 8 428 1.9 ERCP, PTBD, or best supportive care at home.
10
Shigeki et al. 4 84 4.7 It was also noted that among the incidental CaGB patients, four
Present study 5 200 2.5 patients had laparoscopic cholecystectomy in which there are more
chances of biliary spillage. Thus, possibility of the very early disease
becoming a disseminated disease.
Table 11: Comparison of clinical symptoms of GBC by various authors
Weight Nausea/ conclusIon
Series Pain Anorexia Jaundice loss vomiting • In our study, the incidence of incidental CaGB was 2.5%.
Piehler and 76% 34% 38% 39% 32% • Unfortunately, no clinical, biochemical, or radiological
Crichlow parameters were suggestive or predictive of CaGB in patients
Shieh et al. 11 60.4% 43.7% 35.4% 33.3% 35.4% who underwent cholecystectomy for gallstone disease.
Al-Hadeedi et al. 12 47.3% 39.4% 36.4% 39.4% 10.5% • Further analysis revealed incidental CaGB was predominantly a
Shukla et al. 85% 40% 60.3% 14.9% 24.7% disease of elderly female patients. The mean age was 45.4 years
Klamer and Max 13 70% — 40% 40% 30% and 60% of incidental CaGB cases were female.
Silk et al. 14 78.5% 35.6% 28.5% 45.7% 35.6% • In view of the findings from this study, it may be concluded that
chronic cholecystitis remains a significant surgical entity in our
Perpetuo et al. 15 97% — 44% 77% 64% population. However, the suspicion of incidental CaGB should
Kelly and 74% — 32% 48% 51% be borne in mind.
Chamberlain 16 • This is important as laparoscopic cholecystectomy is being
Chao et al. 17 81.1% 4.1% 32.4% 1.4% 16.2% increasingly used for the treatment of chronic cholecystitis.
White et al. 18 83% — 47% 70% — Also, if there is perioperative spillage of biliary contents, there is
Chao and 54.1% 18.9% 45% 28.4% 18.9% a possibility of the very early disease becoming a disseminated
Greager 19 disease. The operating surgeon should have high index of
suspicion regarding this not so uncommon and uniformly fatal
GI malignancy.
No suggestive parameter of incidental CaGB could obtain from
this comparison. Other parameters were also compared, but no result
obtained. Only intraoperative findings are suggestive of CaGB in a orcId
few cases. These findings include adhesions, thickening, irregularity Rahul Omprakash Paliwal https://orcid.org/0000-0003-0654-9419
of GB wall, and disappearance of shiny appearance of gallbladder.
The following parameters of incidental CaGB were compared references
with chronic cholecystitis patients: Among incidental CaGB patients,
mean age was 49.11 years, median age was 47 years, minimum age 1. Shukla VK, Khandelwal C, Roy SK, et al. Primary carcinoma of the gall
bladder: a review of a 16-year period at the University Hospital. J Surg
was 30 years, and maximum age was 76 years. Among incidental Oncol 1985;28(1):32–35. DOI: 10.1002/jso.2930280109.
CaGB cases (n = 5), male patients were 40% and female patients 2. Collier NA, Carr D, Hemingway A, et al. Preoperative diagnosis and its
were 60%. Among incidental CaGB patients, 40% were doing desk effect on the treatment of carcinoma of the gallbladder. Surg Gynecol
job, and 60% were housewives. Among incidental CaGB patients, Obstet 1984;159(5):465–470. PMID: 6208626.
40% were living in urban area and 60% were living in rural area. 3. Kapoor VK. Incidental gallbladder cancer. Am J Gastroenterol
Among incidental CaGB patients, 80% had pain abdomen and 20% 2001;96(3):627–629. DOI: 10.1111/j.1572-0241.2001.03597.x.
had no pain. Among incidental CaGB patients, 40% had nausea and 4. Piehler JM, Crichlow RW. Primary carcinoma of the gallbladder. Surg
Gynecol Obstet 1978;147(6):929–942. PMID: 362580.
20% had vomiting. Among incidental CaGB patients, 0% had weight 5. Weinstein D, Herbert M, Bendet N, et al. Incidental finding of gallbladder
loss. Among incidental CaGB patients, 100% had no jaundice. USG carcinoma. Isr Med Assoc J 2002;4(5):334–336. PMID: 12040819.
was normal (i.e.: only suggestive of chronic cholecystitis) in 100% 6. Tantia O, Jain M, Khanna S, et al. Incidental carcinoma gall bladder
of incidental CaGB cases. during laparoscopic cholecystectomy for symptomatic gall stone
No clinical, biochemical, or radiological parameters were found disease. Surg Endosc 2009;23(9):2041–2046. DOI: 10.1007/s00464-
as preoperative predictor of CaGB in patients who underwent 008-9950-8. PMID: 18443860.
cholecystectomy for chronic cholecystitis. 7. Mittal R, Jesudason MR, Nayak S. Selective histopathology in
There are no characteristic clinical features of EGBC. Unfortunately, cholecystectomy for gallstone disease. Indian J Gastroenterol
2010;29(1):26–30. DOI: 10.1007/s12664-010-0005-4.
it becomes clinically apparent only when it is locally advanced; the 8. Morera Ocón FJ, Ballestín Vicente J, Ripoll Orts F, et al. Cáncer
symptoms being due to invasion of neighboring organs. In two de vesícula biliar en un hospital comarcal [Gallbladder cancer
series, both from areas with a high incidence of GBC, where the index in a regional hospital]. Cir Esp 2009;86(4):219–223. DOI: 10.1016/
of suspicion was high, none of the EGBC was diagnosed clinically j.ciresp.2009.02.021.
World Journal of Laparoscopic Surgery, Volume 14 Issue 3 (September–December 2021) 181