
Page 11 - tmp
P. 11
Surgical Aspects of the Possover LION Procedure
Pneumoperitoneum was formed, an umbilical 12-mm port was tests were employed to ensure lead continuity and placement.
introduced for the camera, and further three 12-mm ports were Leads were then connected to the IPG, which was placed in a
placed in the lower abdomen. subcutaneous pocket on the abdominal wall and firmly fixed
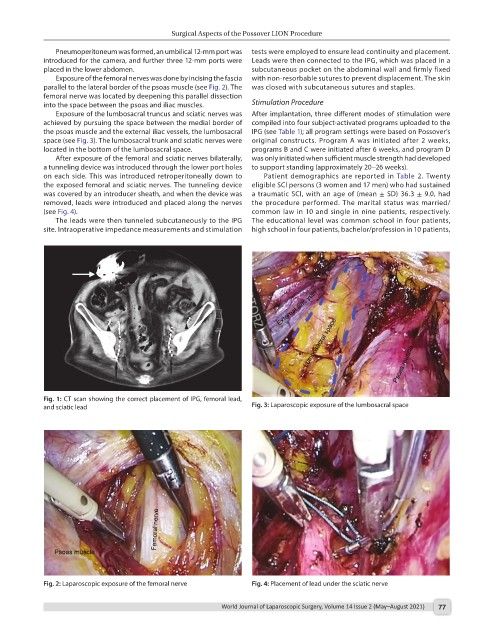
Exposure of the femoral nerves was done by incising the fascia with non-resorbable sutures to prevent displacement. The skin
parallel to the lateral border of the psoas muscle (see Fig. 2). The was closed with subcutaneous sutures and staples.
femoral nerve was located by deepening this parallel dissection
into the space between the psoas and iliac muscles. Stimulation Procedure
Exposure of the lumbosacral truncus and sciatic nerves was After implantation, three different modes of stimulation were
achieved by pursuing the space between the medial border of compiled into four subject-activated programs uploaded to the
the psoas muscle and the external iliac vessels, the lumbosacral IPG (see Table 1); all program settings were based on Possover’s
space (see Fig. 3). The lumbosacral trunk and sciatic nerves were original constructs. Program A was initiated after 2 weeks,
located in the bottom of the lumbosacral space. programs B and C were initiated after 6 weeks, and program D
After exposure of the femoral and sciatic nerves bilaterally, was only initiated when sufficient muscle strength had developed
a tunneling device was introduced through the lower port holes to support standing (approximately 20–26 weeks).
on each side. This was introduced retroperitoneally down to Patient demographics are reported in Table 2. Twenty
the exposed femoral and sciatic nerves. The tunneling device eligible SCI persons (3 women and 17 men) who had sustained
was covered by an introducer sheath, and when the device was a traumatic SCI, with an age of (mean ± SD) 36.3 ± 9.0, had
removed, leads were introduced and placed along the nerves the procedure performed. The marital status was married/
(see Fig. 4). common law in 10 and single in nine patients, respectively.
The leads were then tunneled subcutaneously to the IPG The educational level was common school in four patients,
site. Intraoperative impedance measurements and stimulation high school in four patients, bachelor/profession in 10 patients,
Fig. 1: CT scan showing the correct placement of IPG, femoral lead,
and sciatic lead Fig. 3: Laparoscopic exposure of the lumbosacral space
Fig. 2: Laparoscopic exposure of the femoral nerve Fig. 4: Placement of lead under the sciatic nerve
World Journal of Laparoscopic Surgery, Volume 14 Issue 2 (May–August 2021) 77