
Page 48 - World Journal of Laparoscopic Surgery
P. 48
Postoperative Acute Pancreatitis in a Patient Who Underwent Laparoscopic Cholecystectomy
Fig. 1: Ultrasound showing 2.5 mm thickened gallbladder Fig. 2: MRI of the abdomen showing complex renal mass measuring
28 × 31 mm
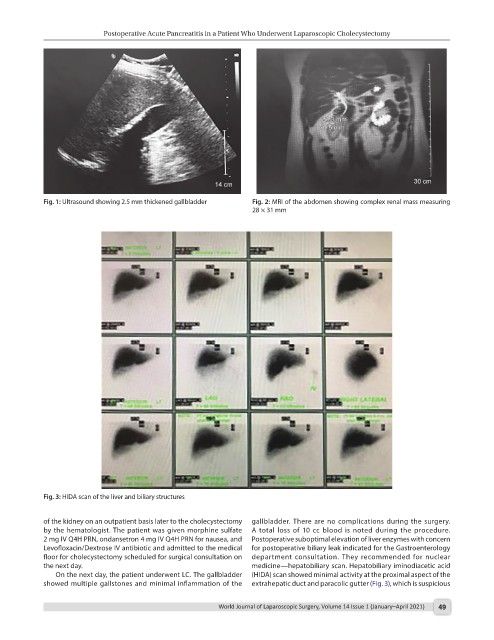
Fig. 3: HIDA scan of the liver and biliary structures
of the kidney on an outpatient basis later to the cholecystectomy gallbladder. There are no complications during the surgery.
by the hematologist. The patient was given morphine sulfate A total loss of 10 cc blood is noted during the procedure.
2 mg IV Q4H PRN, ondansetron 4 mg IV Q4H PRN for nausea, and Postoperative suboptimal elevation of liver enzymes with concern
Levofloxacin/Dextrose IV antibiotic and admitted to the medical for postoperative biliary leak indicated for the Gastroenterology
floor for cholecystectomy scheduled for surgical consultation on department consultation. They recommended for nuclear
the next day. medicine—hepatobiliary scan. Hepatobiliary iminodiacetic acid
On the next day, the patient underwent LC. The gallbladder (HIDA) scan showed minimal activity at the proximal aspect of the
showed multiple gallstones and minimal inflammation of the extrahepatic duct and paracolic gutter (Fig. 3), which is suspicious
World Journal of Laparoscopic Surgery, Volume 14 Issue 1 (January–April 2021) 49