
Page 6 - World Journal of Laparoscopic Surgery
P. 6
Matvey Tsivian et al
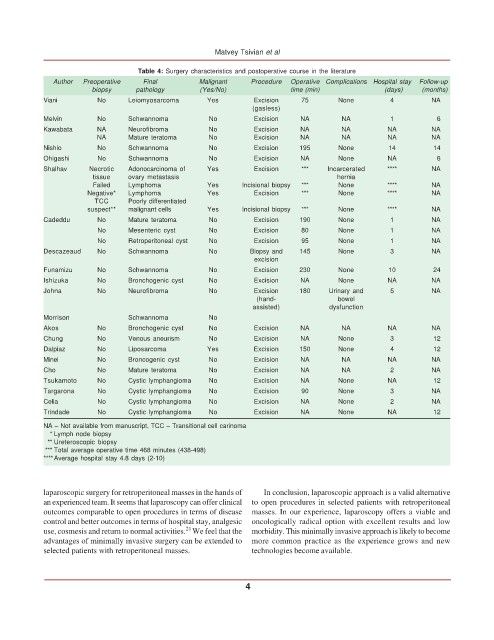
Table 4: Surgery characteristics and postoperative course in the literature
Author Preoperative Final Malignant Procedure Operative Complications Hospital stay Follow-up
biopsy pathology (Yes/No) time (min) (days) (months)
Viani No Leiomyosarcoma Yes Excision 75 None 4 NA
(gasless)
Melvin No Schwannoma No Excision NA NA 1 6
Kawabata NA Neurofibroma No Excision NA NA NA NA
NA Mature teratoma No Excision NA NA NA NA
Nishio No Schwannoma No Excision 195 None 14 14
Ohigashi No Schwannoma No Excision NA None NA 6
Shalhav Necrotic Adonocarcinoma of Yes Excision *** Incarcerated **** NA
tissue ovary metastasis hernia
Failed Lymphoma Yes Incisional biopsy *** None **** NA
Negative* Lymphoma Yes Excision *** None **** NA
TCC Poorly differentiated
suspect** malignant cells Yes Incisional biopsy *** None **** NA
Cadeddu No Mature teratoma No Excision 190 None 1 NA
No Mesenteric cyst No Excision 80 None 1 NA
No Retroperitoneal cyst No Excision 95 None 1 NA
Descazeaud No Schwannoma No Biopsy and 145 None 3 NA
excision
Funamizu No Schwannoma No Excision 230 None 10 24
Ishizuka No Bronchogenic cyst No Excision NA None NA NA
Johna No Neurofibroma No Excision 180 Urinary and 5 NA
(hand- bowel
assisted) dysfunction
Morrison Schwannoma No
Akos No Bronchogenic cyst No Excision NA NA NA NA
Chung No Venous aneurism No Excision NA None 3 12
Dalpiaz No Liposarcoma Yes Excision 150 None 4 12
Minei No Broncogenic cyst No Excision NA NA NA NA
Cho No Mature teratoma No Excision NA NA 2 NA
Tsukamoto No Cystic lymphangioma No Excision NA None NA 12
Targarona No Cystic lymphangioma No Excision 90 None 3 NA
Celia No Cystic lymphangioma No Excision NA None 2 NA
Trindade No Cystic lymphangioma No Excision NA None NA 12
NA – Not available from manuscript, TCC – Transitional cell carinoma
* Lymph node biopsy
** Ureteroscopic biopsy
*** Total average operative time 468 minutes (438-498)
****Average hospital stay 4.8 days (2-10)
laparoscopic surgery for retroperitoneal masses in the hands of In conclusion, laparoscopic approach is a valid alternative
an experienced team. It seems that laparoscopy can offer clinical to open procedures in selected patients with retroperitoneal
outcomes comparable to open procedures in terms of disease masses. In our experience, laparoscopy offers a viable and
control and better outcomes in terms of hospital stay, analgesic oncologically radical option with excellent results and low
21
use, cosmesis and return to normal activities. We feel that the morbidity. This minimally invasive approach is likely to become
advantages of minimally invasive surgery can be extended to more common practice as the experience grows and new
selected patients with retroperitoneal masses. technologies become available.
4